If you've got wrist pain that won't settle, you're probably trying to work out whether it's “just tendonitis” or something more specific like carpal tunnel syndrome. That confusion is common. The symptoms can overlap at first, especially when the problem starts as a vague ache, occasional tingling, or a hand that doesn't feel right after typing, lifting, gripping, or sleeping with your wrist bent.
The important part is this. Carpal tunnel syndrome vs tendonitis is not a minor wording difference. They involve different tissues, they behave differently, and they need different treatment plans. If the diagnosis is wrong, people often spend weeks doing things that don't target the actual problem.
Understanding Your Wrist Pain
Most patients don't arrive saying, “I have median nerve compression,” or, “this is definitely a tendon problem.” They say their hand goes numb when driving, their wrist hurts when lifting a kettle, or they wake at night needing to shake the hand out. Those details matter more than the label you start with.
Carpal tunnel syndrome happens when the median nerve is compressed as it passes through the wrist. Tendonitis is inflammation of a tendon. Those are very different problems, even if both can produce wrist discomfort. The StatPearls overview of carpal tunnel syndrome notes that CTS is the most prevalent focal mononeuropathy, with a general population incidence of 1% to 5%.
That matters for two reasons. First, CTS is common enough that it should always be considered when wrist and hand symptoms include numbness, tingling, or night-time disturbance. Second, common doesn't mean obvious. In clinic, the mistake I see most often is assuming any repetitive-use wrist pain must be tendonitis.
Two different structures, two different signals
A nerve problem usually gives sensory symptoms. That means tingling, pins and needles, altered feeling, or weakness in a recognisable pattern.
A tendon problem usually gives mechanical pain. It tends to hurt with movement, gripping, lifting, or direct pressure over the affected area.
If your symptoms are mainly numbness and tingling, think nerve first. If they're mainly local pain with movement, think tendon first.
What to pay attention to before your appointment
A few observations can make the consultation far more useful:
- Where you feel it: Which fingers are involved matters.
- When it flares: Night symptoms often point in a different direction from activity-only pain.
- What triggers it: Gripping a pan, typing, twisting a jar, or sleeping can all suggest different causes.
- What “pain” means to you: Some patients say “pain” when they really mean burning, tingling, heaviness, or loss of sensation.
That symptom story often gives the first strong clue.
A Look Inside Your Wrist Anatomy
Your wrist is compact, but it handles a crowded job. In clinic, this matters because two problems can sit only millimetres apart and produce very different symptom patterns. One involves a nerve under pressure. The other involves a tendon that is irritated or overloaded.
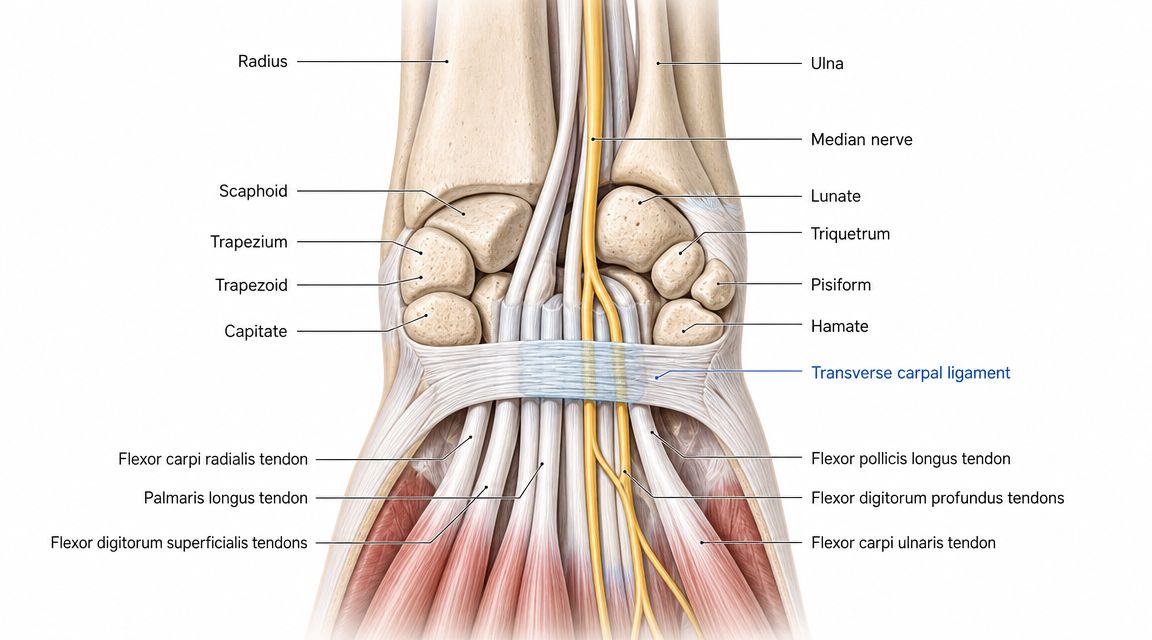
The carpal tunnel in simple terms
The carpal tunnel is a narrow channel at the front of the wrist. Its floor and sides are formed by the wrist bones, and a strong ligament forms the roof. Through that space pass the median nerve and the finger flexor tendons.
Those structures do different jobs. The median nerve carries feeling from part of the hand and helps power some thumb muscles. The tendons transmit force from the forearm muscles to bend the fingers and thumb.
That difference is the starting point for diagnosis.
If the median nerve is compressed, the symptoms usually involve altered sensation, such as tingling, numbness, or a hand that feels clumsy. If a tendon is inflamed or overloaded, the problem is more often pain with motion, gripping, lifting, or direct pressure over the irritated area.
Why nerve symptoms feel different from tendon symptoms
Nerves create a distribution pattern. Tendons create a local pain pattern.
With carpal tunnel syndrome, the median nerve typically affects the thumb, index finger, middle finger, and part of the ring finger. The little finger is usually spared. That detail helps separate carpal tunnel from other wrist and hand conditions, and it is one reason clinicians ask exactly which fingers are involved.
Tendon problems are usually easier to localise. Patients often point to one sore area along the wrist or thumb side and say, "It hurts here when I move." On examination, pain often increases when that tendon is stretched or asked to work against resistance.
This is why a good history and a focused exam matter more than guessing based on the word "wrist pain."
Why this distinction changes treatment
A nerve needs space. A tendon needs load management.
For carpal tunnel syndrome, treatment is aimed at reducing pressure on the median nerve. That may include night splinting, activity changes, guided therapy, injection, or surgical referral if symptoms are persistent or progressing. Patients comparing options for carpal tunnel relief will notice that these plans are built around protecting nerve function.
For tendonitis, the plan is different. The goal is to settle irritation, identify the movement or load that is provoking it, and then rebuild strength and tolerance in a controlled way. A splint that helps one condition can be unhelpful for the other.
The structure involved determines the plan, the expected recovery path, and how urgent it is to get assessed.
Carpal Tunnel vs Tendonitis A Symptom Comparison
A common clinic scenario is this. One patient says, “My hand goes numb when I wake up.” Another says, “It hurts on this exact spot when I lift the kettle.” Both call it wrist pain, but they are describing two different problems, and the treatment plan changes because of that.
Carpal Tunnel vs Tendonitis Key Differentiators
| Symptom | Carpal Tunnel Syndrome | Tendonitis |
|---|---|---|
| Main sensation | Numbness, tingling, pins and needles, weakness | Localised pain, tenderness, soreness |
| Typical location | Thumb, index, middle, and part of ring finger | Over the affected tendon or nearby wrist area |
| Little finger involvement | Usually spared | Can hurt depending on the tendon involved, but not as a nerve pattern |
| Time of day | Often worse at night | Often worse during or after activity |
| Trigger pattern | Wrist position, sustained compression, night-time symptoms | Movement, gripping, lifting, resisted use |
| What patients often say | “My hand goes numb” or “I shake it out at night” | “It hurts when I move it” or “this spot is sore” |
What CTS usually feels like
Carpal tunnel syndrome tends to announce itself through altered feeling rather than one sore point. Patients often describe tingling, numbness, burning, or a hand that feels clumsy and unreliable. Buttons, zips, phone use, and holding a steering wheel can become awkward before strength loss is obvious.
Night symptoms matter here. Waking with tingling or needing to shake the hand out raises suspicion for median nerve compression much more than a simple tendon strain would.
One practical way to separate the two is this. If the complaint is mainly sensory, with numb fingers and pins and needles, carpal tunnel moves higher on the list. If you are already weighing treatment routes, it may help to review options for carpal tunnel relief so the logic behind splints, activity changes, injections, and referral makes sense.
What tendonitis usually feels like
Tendonitis is usually easier to point to with one finger. The pain is often sharp, sore, or pulling, and it tends to appear when the tendon is asked to do work. Gripping, wringing, lifting, twisting a lid, or moving the thumb against resistance often reproduces it.
That pattern matters in practice. A tendon problem usually hurts because it is being loaded. A nerve problem usually causes symptoms because it is being compressed or irritated.
Some tendon conditions also produce stiffness first thing in the morning or a catching sensation with movement. That can worry patients because it feels mechanical. It still differs from the more recognisable numbness pattern of carpal tunnel syndrome.
Common points of confusion
The overlap is where people get stuck.
Pain can occur in both conditions, so pain alone does not settle the diagnosis. Tingling can also coexist with tendon irritation if the whole wrist has been overworked for a period of time. I also see patients with both problems together, especially after repetitive hand use, manual work, childcare, or long hours at a keyboard.
The useful question is not “Does my wrist hurt?” It is “What kind of symptom is it, where exactly do I feel it, and what reliably brings it on?” Those details are what turn a vague complaint into a diagnosis that can guide treatment.
How Doctors Diagnose The Difference
A proper diagnosis starts with listening, not scanning. The history usually tells you where to look before the examination begins.
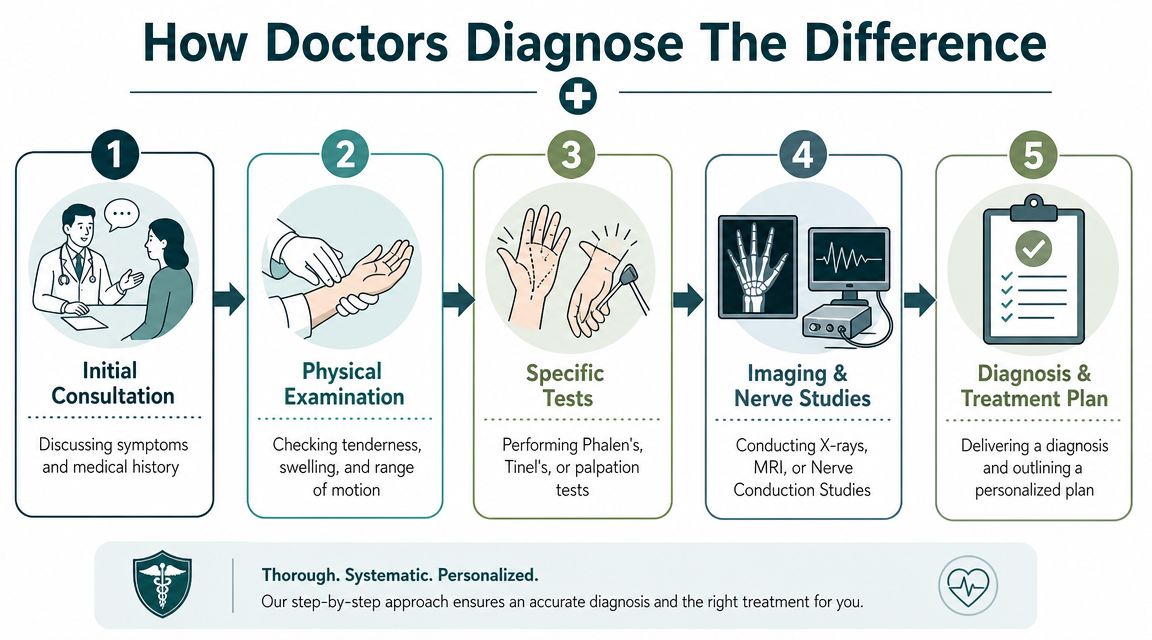
The consultation
A clinician will usually ask questions such as:
- When did it start? Gradual onset often sounds different from a pain that began after one specific task or strain.
- Which fingers are involved? Finger distribution can be a strong clue.
- What wakes you at night? Numbness, pain, and stiffness don't point in exactly the same direction.
- What tasks trigger it? Typing, driving, opening jars, lifting children, using tools, or scrolling on a phone can all matter.
Then comes the examination. With suspected tendonitis, the clinician will often look for local tenderness, swelling, pain on movement, and pain with resisted loading. With suspected carpal tunnel syndrome, the focus shifts towards sensation, provocative wrist positions, and signs of weakness or reduced thumb function.
Specific tests and what they're trying to prove
Tests in clinic aren't magic. They help build or reduce the case for a diagnosis.
For suspected CTS, a doctor may use manoeuvres that provoke median nerve symptoms by changing wrist position or tapping over the nerve. For suspected tendonitis, they'll usually try to reproduce the pain by stressing the tendon in a controlled way and checking exactly where the tenderness sits.
The aim isn't to “catch you out”. It's to see whether the symptoms behave like a compressed nerve or an irritated tendon.
When further tests are useful
If the diagnosis is still uncertain, or symptoms are persistent or severe, further testing may help. In practice, nerve conduction studies are often used when carpal tunnel syndrome needs confirmation, while imaging such as ultrasound can help when the concern is tendon pathology.
Those tests are most helpful when they answer a practical question. Is the nerve compressed? Is there another site of nerve irritation? Is the painful structure a tendon, or something nearby?
A good consultation should leave you with more than a label. You should understand what structure is involved, how confident the diagnosis is, and what the next sensible step looks like.
Comparing Treatment Pathways and Options
The treatment split between carpal tunnel syndrome vs tendonitis is where the diagnostic accuracy really earns its value. If you treat nerve compression like a load problem, or a tendon problem like a nerve problem, progress tends to stall.
First-line treatment is not the same
Management strategies differ. For CTS, treatment such as splinting or surgery aims to decompress the median nerve. For tendonitis, management is load-driven, focusing on rest and progressive rehabilitation to restore tendon capacity, as discussed in this mechanistic and management review on CTS treatment.
In plain terms:
- CTS treatment goal: create more comfort for the nerve and reduce ongoing compression.
- Tendonitis treatment goal: reduce irritation, then rebuild the tendon's tolerance to use.
What often works for carpal tunnel syndrome
For mild or early CTS, practical treatment may include:
- Neutral wrist splinting: Especially at night, to avoid prolonged wrist positions that irritate the median nerve.
- Activity modification: Reducing tasks that keep the wrist bent or under repeated compressive strain.
- Ergonomic correction: Keyboard, mouse, grip tools, and workstation height can all matter.
- Escalation when needed: If symptoms persist, weakness develops, or numbness becomes more constant, steroid injection or surgical decompression may be considered.
If you're comparing braces or temporary support options before review, these wrist supports and arthritis gloves can give you a sense of the types patients commonly use, though the right choice still depends on the diagnosis.
What often works for tendonitis
Tendonitis responds better to a different strategy:
- Calm it down first. That may mean short-term rest from the aggravating task, icing, compression, or a temporary splint depending on the tendon involved.
- Stop repeatedly provoking it. A frequent mistake involves continuing the same painful gripping or lifting pattern daily, which prevents the tendon from settling.
- Rebuild capacity gradually. Once pain is quieter, progressive rehabilitation matters. Complete avoidance for too long can leave the tendon weaker and more irritable when activity restarts.
What doesn't work well
A few common mistakes delay recovery:
- Using any brace without a reason: The wrong support can be uncomfortable or irrelevant.
- Pushing through numbness: That's risky if the underlying issue is nerve compression.
- Resting tendonitis forever: Short-term unloading can help, but long-term avoidance usually doesn't restore function.
- Treating only the pain: Pain relief matters, but the underlying mechanical or neurological driver still needs addressing.
Good treatment feels targeted. You should know whether the plan is trying to unload a tendon or decompress a nerve.
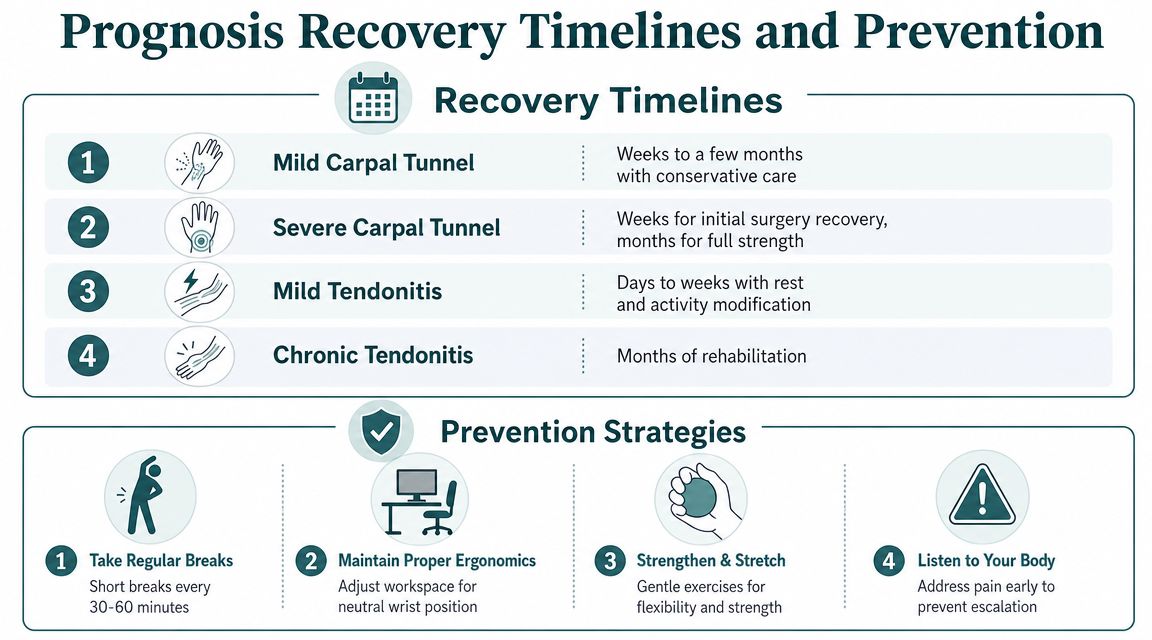
Prognosis Recovery Timelines and Prevention
Two practical questions often arise. How long will this take, and how do I stop it coming back?
Recovery depends on severity, duration, and whether the diagnosis is right from the start. A mild tendon flare can settle relatively quickly if the irritating activity is reduced early. A longer-standing tendon problem often needs a more patient rehabilitation phase. Carpal tunnel syndrome also varies. Some people improve with splinting and activity changes, while others need a more definitive decompression pathway before symptoms properly settle.
What recovery usually depends on
The patients who do best tend to get three things right:
- They address the correct diagnosis early.
- They stop repeating the exact aggravating pattern.
- They follow through once symptoms ease, rather than abandoning the plan too soon.
That last point matters. A wrist that feels better isn't always a wrist that's ready for full workload.
Prevention that actually helps
Prevention isn't about avoiding all hand use. It's about reducing the repeated strain that keeps tipping the wrist over the edge.
- Take regular breaks: Short pauses during prolonged typing, gripping, or tool use can reduce cumulative strain.
- Keep the wrist more neutral: Workstation setup, mouse position, keyboard angle, and how you hold a phone all influence wrist posture.
- Vary the task: Repeating one motion for long periods is harder on both tendons and nerves than changing position and load.
- Build capacity: Gentle strengthening and mobility work can make the wrist more resilient when reintroduced sensibly.
- Act early: A problem that is mild and intermittent is much easier to manage than one that has become constant.
If you want practical self-management ideas around splints, pacing, and comfort measures, you can discover MEDISTIK wrist health tips as a useful starting point.
The best prevention plan is specific to the task that causes your symptoms. “Use your hands less” isn't realistic advice for most people.
A realistic expectation
Improvement is rarely completely linear. Symptoms often ease, flare slightly with a return to activity, then improve again once the workload is adjusted properly. That doesn't always mean treatment has failed. It usually means the wrist is telling you where its current limit is.
When You Should See a Specialist
Some symptoms deserve prompt review rather than watchful waiting. If you have persistent numbness, increasing weakness, dropping objects, difficulty with simple hand tasks, or visible loss of muscle at the base of the thumb, it's sensible to seek specialist assessment. The same applies if pain is not settling, keeps returning, or the diagnosis remains unclear after initial treatment.
A specialist consultation helps in two ways. First, it narrows the diagnosis properly. Second, it stops you wasting time on the wrong treatment. That matters if you use your hands for work, childcare, sport, or daily tasks you can't pause.
If you'd like a faster route to assessment, investigation, and consultant-led treatment, Haven Medical offers private access to wrist and hand evaluation, including carpal tunnel pathways and day surgery where appropriate. If your symptoms fit the patterns described above and you want clarity, visit website to learn more, call to book a consultation, or click to book if you're ready to be seen.
A clear diagnosis is what changes everything. Once you know whether the problem is nerve compression or tendon irritation, the treatment plan becomes much more straightforward.