Eczema is one kind of dermatitis. Dermatitis is the broader medical term for inflamed skin. In everyday UK practice, people often use the words as if they mean the same thing, which is why many patients arrive unsure whether they have one condition, two different diagnoses, or a rash that has been labelled in different ways.
A common clinic scenario is someone with itchy, dry, sore skin who has already tried changing soaps, buying a moisturiser, and searching online for answers. What usually helps most is getting the name right first. Once you know whether the problem fits eczema, contact dermatitis, seborrhoeic dermatitis, or something else entirely, treatment becomes much more targeted.
That clarity matters. A private dermatology assessment can often speed things up, especially if you want a careful history, a close skin examination, and a treatment plan customized to your triggers, routine, and previous flare-ups.
The Itchy Question Eczema or Dermatitis
You notice an itchy patch on your eyelids, hands, or behind your knees, and the label becomes the confusing part. One person says eczema. Another says dermatitis. An online search adds psoriasis, allergy, dry skin, and stress rash to the mix.
In clinic, this is one of the commonest points of confusion, and the wording matters because the words are related but not interchangeable. If the names feel blurry, the simplest way to clear them up is to sort the broad term from the specific diagnosis.
Why the terms get mixed up
Dermatitis is the medical term for inflamed skin. It works like an umbrella label.
Eczema usually means atopic dermatitis, which is one particular type under that umbrella.
That distinction helps in a practical way. If you are told you have dermatitis, you know the skin is inflamed, but you still need the next layer of detail. Is it atopic eczema, contact dermatitis, seborrhoeic dermatitis, or something else that only looks similar at first glance?
If you are told you have eczema, that usually points to a more recognisable pattern. It often involves dry, sensitive skin, itching, and flare-ups that settle and return over time.
Main takeaway: If you're comparing eczema vs dermatitis, you're comparing a broad medical category with one common subtype inside it.
A useful comparison is fever and infection. Fever tells you something is going on, but not the exact cause. In the same way, dermatitis tells you the skin is inflamed. Eczema tells you more about the pattern of that inflammation.
This is why self-diagnosis can go wrong so easily. A rash from frequent handwashing, a reaction to fragrance, and atopic eczema can all look red, dry, and sore, especially in the early stages. Yet the treatment plan may differ quite a lot. Someone with contact dermatitis may need trigger avoidance and, in some cases, patch testing. Someone with atopic eczema may need a longer-term skin barrier plan with regular emollients and flare control.
In the UK, this terminology often gets blurred in everyday conversation, even though getting the label right is what leads to the right treatment. A private dermatology appointment can be particularly helpful here. You have time to go through where the rash started, how it behaves, what products or exposures may be involved, and whether the pattern fits eczema or another form of dermatitis. That kind of clarity often shortens the trial-and-error phase and gets you to a more personal treatment plan sooner.
Defining Dermatitis The Umbrella Term for Skin Inflammation
Dermatitis is a medical umbrella term. It doesn't name one single disease. It describes a group of skin conditions where the skin becomes inflamed.
That inflammation can show up in several ways. The exact look varies from person to person, but the common features are familiar.
What dermatitis usually looks like
You might notice:
- Redness or colour change
- Itching that can range from mild to intense
- Dry, flaky, or rough skin
- Swelling, stinging, or tenderness
- Blistering, oozing, or cracking in some cases
Some rashes stay localised. Others spread. Some come on quickly after exposure to a product or material. Others linger and become chronic.
To make the relationship clearer, this visual helps:
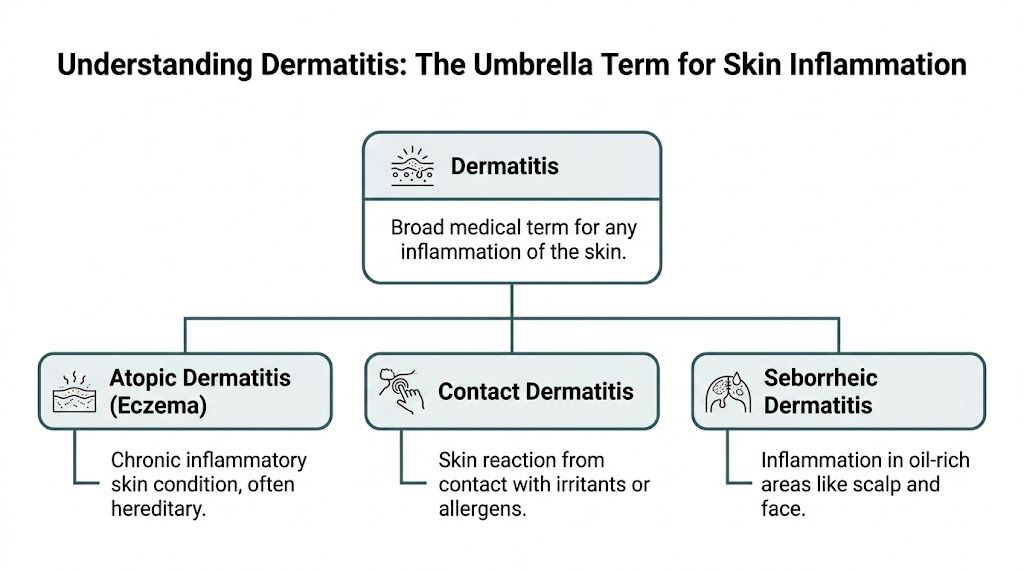
Common types of dermatitis
The main types patients often hear about include:
- Atopic dermatitis. This is the form commonly referred to as eczema. It tends to be long-term, itchy, and linked with sensitive, dry skin.
- Contact dermatitis. This happens when the skin reacts to something it touches. That could be an irritant, such as repeated exposure to soap or cleaning products, or an allergen, such as fragrance, nickel, or preservatives.
- Seborrhoeic dermatitis. This often affects oil-rich areas such as the scalp, sides of the nose, eyebrows, ears, or chest. It can look flaky, greasy, or inflamed.
A patient might say, "I have dermatitis on my scalp," and mean seborrhoeic dermatitis. Another might say, "I have dermatitis on my hands from work gloves," and mean contact dermatitis. Another may have had itchy flexures since childhood and have atopic dermatitis, or eczema.
Clinical rule: “Dermatitis” is the broad category. The useful part of the diagnosis is identifying which type sits underneath it.
That distinction is where the treatment starts to become sensible. A broad label can describe the problem. A specific diagnosis helps solve it.
Key Differences and Similarities Explained
The reason patients search for eczema vs dermatitis is that the overlap is real. From the outside, both can itch, sting, flake, redden, and interfere with sleep, concentration, and confidence.
Where they overlap
Both eczema and other forms of dermatitis can involve:
- Itching
- Dryness
- Visible inflammation
- Irritation after environmental exposure
- Worsening with stress, heat, or friction
From a patient perspective, they can feel almost identical. That's why self-diagnosis often goes wrong. The skin may look broadly similar while the underlying reason is very different.
Where the difference matters
The key distinction is scope.
Dermatitis is a general category. It includes multiple inflammatory skin conditions with different causes.
Eczema, in everyday use, usually means atopic dermatitis. That is a specific subtype, and it often follows a recurring pattern over time.
Here is the simplest way to compare them:
Eczema vs Dermatitis At a Glance
| Feature | Dermatitis (General Term) | Eczema (Atopic Dermatitis) |
|---|---|---|
| Meaning | Broad term for skin inflammation | A specific type of dermatitis |
| Scope | Includes several different conditions | One subtype within the dermatitis group |
| Common causes | Can be irritant, allergic, environmental, or other triggers | Often linked to genetic tendency, immune sensitivity, and skin barrier problems |
| Pattern | May be short-term or ongoing, depending on type | Often chronic, with flare-ups and remissions |
| Typical examples | Contact dermatitis, seborrhoeic dermatitis, atopic dermatitis | Atopic dermatitis |
| Family history | May or may not be relevant | More often associated with asthma, allergies, or hay fever in the family |
| Main clinical question | What kind of dermatitis is it? | How active is the eczema, and what is triggering flares? |
A practical example helps. If your rash appeared after wearing a watch strap or using hair dye, a clinician may think first about contact dermatitis. If you’ve had recurrent itchy dry skin since childhood, particularly in typical areas, eczema becomes more likely.
All eczema is dermatitis, but not all dermatitis is eczema.
That one sentence clears up most of the confusion. The next step is understanding why one person develops atopic eczema while another reacts to a soap, glove, metal, or shampoo.
Understanding the Causes and Triggers of Itchy Skin
Eczema doesn’t happen for one simple reason. In atopic dermatitis, the skin barrier, the immune system, and inherited tendency all interact.
A useful analogy is a brick wall. Healthy skin works like a well-built wall, keeping moisture in and irritants out. In eczema, that wall is less secure. Water escapes more easily, and outside triggers get in more easily.
Why atopic eczema behaves differently
One of the best-known biological factors involves the filaggrin gene, often shortened to FLG. Filaggrin helps the outer skin barrier stay organised and hold onto moisture.
In atopic eczema, FLG gene mutations have been identified in up to 56% of patients with moderate-to-severe disease, and carriers have 3.1 times higher odds of developing eczema by age 3. These changes weaken the barrier and make it easier for allergens to penetrate and trigger inflammation (filaggrin and eczema overview).
So when a patient says, “My skin reacts to everything,” that isn’t always an exaggeration. If the barrier is impaired, ordinary exposures can feel much less ordinary.
What tends to trigger flares
For atopic eczema, common aggravating factors often include:
- Dry environments and overheated rooms
- Harsh soaps, fragranced products, and detergents
- Rough fabrics or friction
- Stress
- Illness or general skin irritation
Bedding and fabric choice can matter too, especially if heat and friction make night-time itching worse. Patients who are reviewing sleep comfort often find practical guidance in resources such as best bed sheets for sensitive skin, particularly when trying to reduce irritation from coarse or overly warm materials.
Other types of dermatitis have different roots
Not all dermatitis starts from an inherited barrier problem.
With irritant contact dermatitis, the skin becomes inflamed because something repeatedly damages it. Frequent handwashing, sanitisers, cleaning products, hair chemicals, and wet work are classic examples.
With allergic contact dermatitis, the issue is immune recognition of a specific substance. Nickel in jewellery, fragrance in skincare, preservatives in creams, or ingredients in nail and hair products can all be relevant.
Seborrhoeic dermatitis follows a different pattern again. It usually affects oily areas such as the scalp and face and often causes flaky, inflamed patches rather than the classic dry flexural eczema pattern.
The visible rash may look similar enough to confuse patients. The cause underneath is what changes the plan.
How a Specialist Diagnoses Your Skin Condition
A proper diagnosis isn’t just a quick glance across the desk. Dermatology is pattern recognition, history-taking, and knowing which questions matter.
What happens in a real assessment
A specialist usually starts by asking about timing and pattern. Did the rash begin in childhood or adulthood? Is it always in the same place? Does it worsen after work, after certain products, or in winter? Is there a personal or family history of asthma, hay fever, or sensitive skin?
Then comes the examination. Distribution matters. So does texture. A rash on the eyelids has a different list of likely causes from a rash on the scalp or between the fingers.
Useful questions often include:
- When did it start
- Where does it appear first
- What products touch the area
- Is the itch affecting sleep
- Has anything clearly made it worse or better
- Are there signs of infection such as pain, crusting, or weeping
When testing is needed
Not every patient needs tests. Many diagnoses are clinical. But if contact allergy is suspected, patch testing may help identify whether a substance such as fragrance, nickel, or preservatives is driving the rash.
Patch testing is especially helpful when the pattern doesn’t fit straightforward eczema, or when treatment keeps failing because the trigger is still being applied every day without realising it.
A cream can’t solve a problem if the real cause is still sitting on your skin, scalp, jewellery, gloves, or shampoo bottle.
Why expertise matters across skin tones
Diagnosis can be harder in skin of colour, where eczema may present differently and classic textbook descriptions may be less obvious. That difference matters. Delayed recognition leads to delayed relief.
A UK-focused resource on eczema in skin of colour notes that only half of minority children with severe eczema receive appropriate treatment, and it highlights the risk of misdiagnosis or delay without culturally informed assessment (eczema in skin of colour clinical resource).
If you’re unsure what your rash is, that uncertainty is itself a reason to get assessed. The most effective treatment usually follows the most accurate name.
Your Eczema and Dermatitis Treatment Options in the UK
Treatment only works well when it matches the diagnosis. That’s why dermatitis treatment UK searches often produce mixed advice. Some recommendations are meant for eczema. Others are designed for contact allergy or scalp dermatitis.

Treatments many patients start with
For many inflammatory rashes, the basics still matter:
- Emollients help restore and protect the skin barrier. Ointments, creams, and lotions each suit different people and body sites.
- Topical corticosteroids calm inflammation during flares.
- Trigger avoidance reduces the cycle of damage and re-irritation.
For eczema, consistency matters more than occasional bursts of treatment. A patient who moisturises only when the skin is already flaring is often always trying to catch up.
Some people also explore texture and routine changes that make moisturising easier to stick with. For example, parents and adults comparing oil-based options may find a practical discussion in this guide to body oil eczema solution, especially if standard creams feel difficult to use regularly.
How treatment differs by diagnosis
If the problem is atopic eczema, the long-term plan usually includes ongoing skin care, flare treatment, and review of aggravating factors. Some patients need prescription creams beyond standard moisturisers, and some benefit from more advanced therapies under specialist care.
If the problem is contact dermatitis, the most important treatment may be identifying and avoiding the culprit. A strong cream may settle the rash temporarily, but it often returns if the trigger stays in daily life.
If the problem is seborrhoeic dermatitis, treatment often focuses on scalp or facial management with targeted products for those areas, not a generic “eczema cream” approach.
Severity changes the plan
Severity matters too. The 2017 NICE guidelines on atopic eczema identified 20 to 30% of paediatric diagnoses as moderate-to-severe, and modern consultant-led therapies can reduce severe sleep-disturbing symptoms from 2 to 4% of cases to under 1% (NICE-related eczema summary).
That’s important because poor sleep changes everything. Children become miserable and irritable. Adults lose concentration, scratch unconsciously, and dread bedtime. Good treatment isn’t just about appearance. It’s about comfort, rest, and getting normal life back.
Practical advice: If your current treatment gives only brief relief, the problem may not be that your skin is “stubborn”. The diagnosis, strength, application method, or trigger list may need revisiting.
When to Book an Assessment with a Private Dermatologist
You start with a dry, itchy patch and assume it will calm down on its own. A few weeks later, it is still there, you are sleeping badly, and you have a bathroom shelf full of creams that have not really answered the question of what the rash is.
That is often the point when a specialist assessment becomes useful.
In clinic, one of the commonest sources of delay is not laziness or poor skin care. It is uncertainty. People are told they have “eczema”, “dermatitis”, “sensitive skin”, or even “an allergy”, as if these all mean the same thing. They do not. In the UK, getting the label right matters because the next step may be prescription treatment, patch testing, infection treatment, or practical advice about work exposures.
Signs you shouldn’t ignore
Consider specialist advice if:
- Sleep is being affected by scratching, stinging, or discomfort
- The skin looks infected, with weeping, crusting, increasing pain, or tenderness
- The rash involves the face, eyelids, hands, or genital skin, where the diagnosis and treatment choice need extra care
- Work seems to trigger it, especially if you handle soaps, chemicals, gloves, hair products, or cleaning agents
- You’ve tried over-the-counter creams repeatedly and the rash keeps coming back
- You’re confused about whether this is eczema, dermatitis, allergy, or something else
A private dermatologist can often add value when speed and precision matter. That may mean reviewing a rash before it spreads further, deciding whether patch testing should be considered, or separating eczema from contact dermatitis, psoriasis, fungal infection, or another lookalike condition.
The main benefit is clarity. Instead of trying one more cream and hoping for the best, you get a diagnosis that fits the pattern of your skin, your triggers, and your day-to-day life. For many patients in the UK, that shorter path to an answer is the difference between ongoing guesswork and a treatment plan that makes sense.