If you’re dealing with skin that stays red, flaky, sore, or itchy no matter how much moisturiser you use, it’s understandable to feel worried. Many people first assume it’s dry skin, eczema, irritation, or an allergy. When it keeps returning in the same places, starts scaling, or begins to affect your scalp, nails, or confidence, it often needs a closer look.
Psoriasis can feel visible in a way few other conditions do. It can affect how comfortable you feel in your clothes, how you sleep, and how willing you are to show your skin. The reassuring part is that it is manageable, and effective treatment usually starts with getting the diagnosis right.
What Is Psoriasis and How Common Is It in the UK?
Psoriasis is a chronic autoimmune skin condition. That means your immune system becomes overactive and drives skin cells to build up too quickly. Instead of shedding gradually, skin cells collect on the surface and form the raised, inflamed, scaly areas often called plaques.
This is why psoriasis is more than “just dry skin”. Dry skin can flake. Psoriasis tends to create thicker, more defined patches, often with noticeable scaling and inflammation. It can also come and go in cycles, with calmer periods followed by flare-ups.
Why the skin looks different
Healthy skin renews itself steadily. With psoriasis, that process speeds up too much. It’s like a conveyor belt moving faster than your skin can clear away old cells. The result is a visible build-up.
Psoriasis isn’t caused by poor hygiene, and it isn’t something you can catch from someone else. For many newly diagnosed patients, hearing that matters. Skin conditions still carry stigma, and psoriasis often affects confidence as much as comfort.
Practical rule: If a rash is recurring, sharply outlined, scaly, or not settling with basic skincare, it’s worth getting a proper skin assessment rather than guessing.
How common psoriasis is in the UK
Psoriasis is common in everyday clinical practice. In the United Kingdom, it affects approximately 1.52% of the general population, according to research published in the National Library of Medicine.
That same research also found that psoriasis is more common in people with a higher body mass index, lower physical activity levels, and smoking habits. It also noted that self-reported lifetime prevalence more than doubled over a 29-year period, which reflects a growing need for effective long-term management.
A simple way to interpret that is this. If you’ve just been told you have psoriasis, you’re not dealing with something rare or obscure. It’s a recognised medical condition that clinicians see regularly, and there are established ways to manage it.
The key point to remember
Psoriasis is long term, but it doesn’t mean you’ll always feel as you do during a flare. Many people do well once they understand their triggers, get the right treatment for the type they have, and review things early when symptoms change.
Understanding Psoriasis Symptoms and Types
Plaque psoriasis is often the first form observed. It is the most common type, accounting for 80% to 90% of cases, as summarised in this psoriasis facts overview.
Here is the visual guide many patients find helpful:
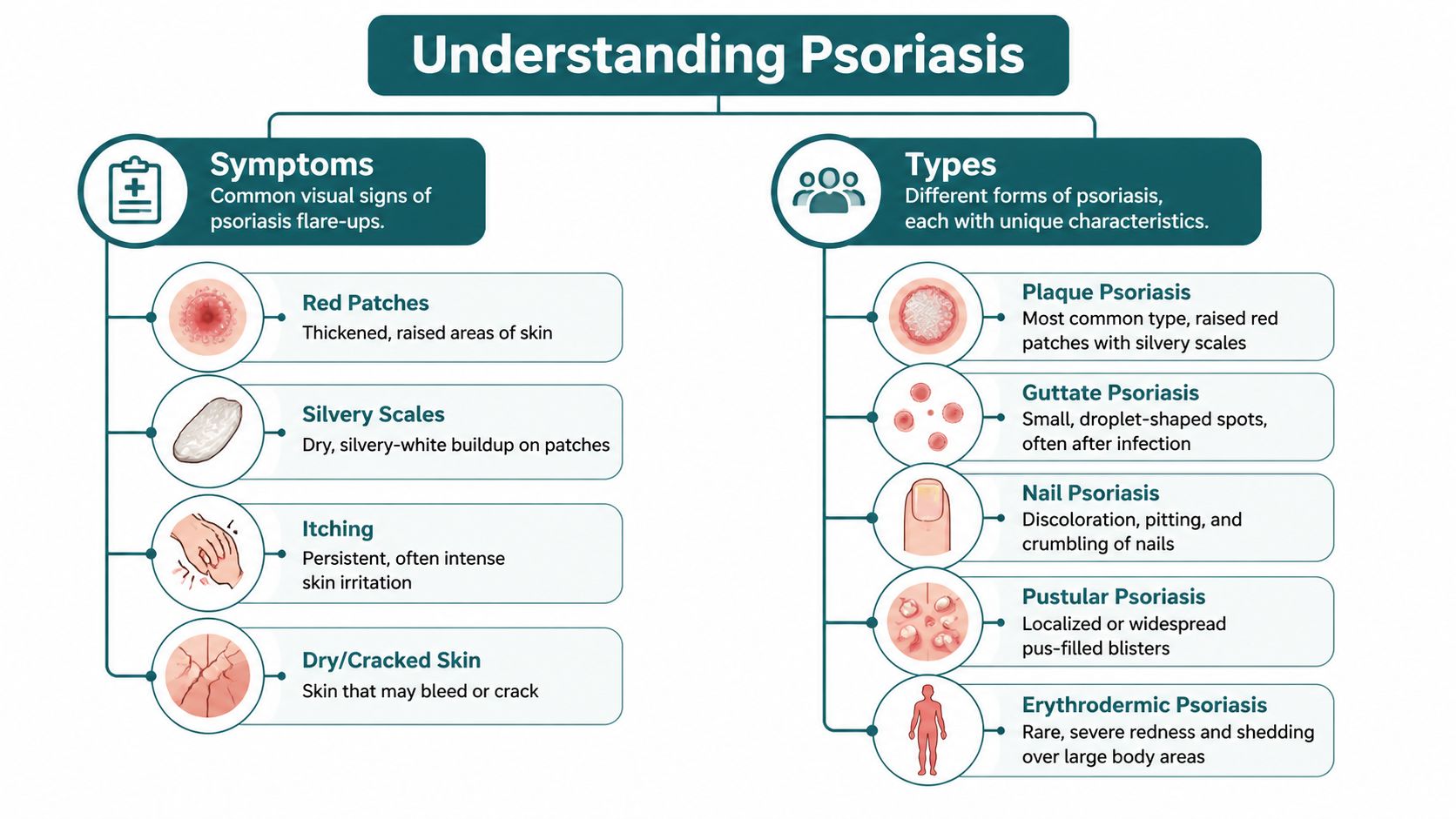
Common psoriasis symptoms
You might notice:
- Red, inflamed patches that look well defined rather than vague or blotchy
- Silvery-white scale sitting on top of the affected skin
- Dry or cracked areas that may sting or bleed
- Itching, burning, or soreness that ranges from mild irritation to real discomfort
On darker skin tones, psoriasis may not always look bright red. It can appear darker, more violet-toned, or differently pigmented, which is one reason it can sometimes be missed or mistaken for another condition.
Common areas affected
Psoriasis often shows up in places that experience friction or repeated pressure. Typical sites include:
- Elbows and knees
- Scalp
- Lower back
- Hands and feet
- Nails
Some areas are especially frustrating because they affect daily life more directly. Scalp psoriasis can shed visibly onto clothing. Nail psoriasis can change the appearance and texture of nails. Psoriasis on the hands, feet, face, or genital area can feel particularly distressing and may need an individualized treatment plan.
Other types of psoriasis
Not all psoriasis looks the same. A few examples:
- Guttate psoriasis often appears as smaller drop-like spots.
- Inverse psoriasis tends to affect skin folds and can look smoother and less scaly because of moisture and friction.
- Pustular psoriasis causes pus-filled bumps and needs medical review.
- Erythrodermic psoriasis is rare and severe, involving widespread redness and shedding.
A symptom pattern can overlap with fungal rashes, eczema, seborrhoeic dermatitis, or contact dermatitis. That’s why self-diagnosis is often unreliable, especially if the rash is on the scalp, face, or in skin folds.
Symptoms beyond the skin
Psoriasis can involve more than the visible plaques. The same source notes that scalp psoriasis affects 45% to 56% of people with psoriasis, nail psoriasis occurs in about 50%, and psoriatic arthritis develops in up to 30%.
If you have psoriasis and also notice stiff, painful, or swollen joints, mention it promptly. Joint symptoms should never be brushed aside as unrelated.
A new diagnosis often brings one simple question. “Does this sound like me?” If the answer is even “possibly”, a proper dermatology review is more useful than trying one product after another and hoping something works.
What Causes Psoriasis Flare-Ups
Psoriasis develops because the immune system sends the wrong signals to the skin, causing it to regenerate much faster than it should. New skin cells rise to the surface before the older ones have had time to shed properly. That is why plaques build up, scale appears, and the skin can become red, thick, itchy, or sore.
For many people, the harder part is not understanding the biology. It is understanding why the skin can seem fairly settled one month, then suddenly worsen after a stressful week, an illness, or even a small injury. Psoriasis often behaves that way. There is usually an underlying tendency in the body, then everyday triggers push the skin into a flare.
What sits behind it
Psoriasis has an autoimmune basis, and genes often influence who develops it. Some people know there is a family history. Others are the first in the family to be diagnosed.
Two points often bring real relief. You did not cause psoriasis by poor hygiene, and you cannot give it to someone else through touch. It is understandable to feel self-conscious about visible plaques, especially around partners, hairdressers, or at the gym, but psoriasis is not contagious.
Common flare triggers
A trigger does not create psoriasis from nothing. It acts more like a switch that turns up inflammation in skin that is already prone to it. Common triggers include:
- Stress. Emotional pressure can make immune activity more reactive and may worsen a flare.
- Infections. Sore throats and other infections can bring psoriasis on suddenly or make existing plaques worse.
- Skin injury. Cuts, scratching, shaving nicks, tight clothing, friction, or sunburn can cause psoriasis to appear in that exact area. Clinicians call this the Koebner phenomenon.
- Certain medicines. Some treatments can aggravate psoriasis in people who are susceptible.
- Cold, dry weather. Winter often dries and irritates the skin, which can make symptoms more active.
Triggers differ from person to person. One patient may flare after a throat infection. Another notices problems after stress and poor sleep. A third mainly struggles in winter.
Why trigger tracking helps
You do not need to analyse every patch of skin. A simple pattern is enough. If you note when a flare started, where it appeared, and what was happening around that time, your clinician can often spot trends much faster.
This matters in the UK because waiting for routine NHS dermatology review can take time, while a flare is affecting you now. Faster access to a dermatologist can mean earlier confirmation of triggers, quicker treatment changes, and a plan customized to your skin rather than more weeks of trial and error. For patients who need answers sooner, private dermatology through Haven Medical can be a practical way to get that personalised care without a long delay.
Good psoriasis care includes treating the skin in front of you and working out what repeatedly pushes it into flare mode.
How Psoriasis Is Diagnosed in the UK
For many people, the hardest part is the uncertainty before diagnosis. They know something isn’t right, but they don’t know whether it’s psoriasis, eczema, fungal infection, dermatitis, or something else. The good news is that diagnosis is often straightforward when an experienced clinician examines the skin properly.
In the UK, psoriasis is usually diagnosed clinically. That means a GP or dermatologist looks closely at the skin, scalp, and nails, asks about symptoms, and considers the overall pattern.

What a clinician will usually ask
The consultation is rarely complicated. Expect questions such as:
- When did it start
- Does it itch, sting, crack, or bleed
- Has it appeared in the same places before
- Do you have any nail changes
- Do you have joint pain or morning stiffness
- Does anyone in your family have psoriasis or another skin condition
- Did it flare after illness, stress, or a new medicine
These questions help separate psoriasis from lookalike conditions. A sharply demarcated rash on the elbows and scalp points in a different direction from a short-lived allergic rash or a fungal infection in a skin fold.
Is a biopsy always needed?
Usually, no. In many cases, the appearance and distribution are enough. If the rash is unusual, mixed with another skin problem, or not responding as expected, a clinician may suggest a skin biopsy.
A biopsy means taking a very small sample of skin after numbing the area. Patients often worry this sounds dramatic, but in practice it is a minor procedure used when the diagnosis needs clarification.
Why timing matters
Psoriasis isn’t only about what is visible today. Diagnosis affects treatment choices, symptom control, and whether related issues such as nail disease or possible psoriatic arthritis are picked up early.
Some people are diagnosed quickly. Others wait while trying repeated creams that don’t fit the problem. If your rash is persistent, spreading, or affecting your sleep, work, scalp, or hands, getting specialist input sooner can make a real difference.
A clear diagnosis often brings relief in itself. Once you know what you’re dealing with, treatment becomes far more targeted.
Evidence-Based Psoriasis Treatment Options
Psoriasis treatment isn’t one-size-fits-all. Doctors usually choose treatment based on how extensive the psoriasis is, which body sites are involved, how uncomfortable it feels, and how much it affects daily life. The recognised approach is hierarchical, with stronger or more targeted treatments used when needed.
According to the American Academy of Dermatology psoriasis guidance, topical corticosteroids are first-line therapy for mild to moderate plaque psoriasis, and steroid-sparing agents are important for chronic management. That same guidance also notes that treatment success should be assessed not only by disease severity but also by patient-reported tools such as the Dermatology Life Quality Index (DLQI).

First-line options for milder psoriasis
For many patients, treatment starts with creams, ointments, or scalp preparations.
| Treatment type | How it helps | Practical point |
|---|---|---|
| Emollients | Soften scale and reduce dryness | Best used consistently, not only during flares |
| Topical corticosteroids | Calm inflammation and reduce redness and itch | Usually used in courses and with supervision if longer term |
| Vitamin D analogues | Help slow excess skin cell production | Often useful as steroid-sparing treatment |
| Other topical agents | May include tazarotene, calcineurin inhibitors, salicylic acid, anthralin, or coal tar | Choice depends on body site and skin sensitivity |
Delicate areas such as the face, groin, skin folds, palms, soles, scalp, and nails often need more careful planning. A treatment that works well on the elbow may be too irritating or too strong for another site.
When treatment needs to step up
If psoriasis is more widespread, keeps relapsing, or affects difficult areas, clinicians may recommend phototherapy or systemic treatment.
- Phototherapy uses controlled ultraviolet light under medical supervision.
- Oral systemic medicines may be used when topical treatment isn't enough.
- Biologic therapies target specific parts of the immune system and can be appropriate for more severe disease or for people with related joint involvement.
Patients sometimes think moving beyond creams means their psoriasis is “very bad”. That's not always true. It may mean the location, persistence, or impact on quality of life justifies a different approach.
Quality of life matters in treatment decisions
This is a point many people don't hear early enough. Psoriasis severity isn't judged only by how much skin is covered. A smaller area on the scalp, face, hands, feet, or genitals can affect life far more than a larger patch hidden under clothing.
Doctors increasingly use patient-reported measures because symptoms such as itching, visible flaking, sleep disruption, embarrassment, and discomfort at work matter. If your skin is affecting how you function, that should be part of the treatment conversation.
Small areas can still deserve serious treatment if they interfere with daily life.
Access barriers can shape treatment just as much as symptoms
In real life, not everyone reaches advanced treatment at the same speed. Access, confidence, cost concerns, stigma, and how quickly someone sees a specialist all play a role. Some patients also need more culturally sensitive support, especially when skin signs appear differently across skin tones or when there are concerns about long-term medicines.
Good psoriasis care means more than writing a prescription. It means reviewing whether the diagnosis is right, whether the treatment matches the body site, whether the plan is realistic for your routine, and whether you're getting enough relief.
Living Well with Psoriasis and Managing Your Health
Living with psoriasis often means learning two skills at once. The first is how to treat the skin. The second is how to protect your confidence and routine when the condition flares.
That balance matters because psoriasis can be physically uncomfortable and emotionally draining. A flare on the scalp may leave visible shedding on dark clothing. A flare on the hands may make you self-conscious during meetings, handshakes, or everyday tasks.
Daily habits that support calmer skin
The basics aren't glamorous, but they do help.
- Keep moisturising simple. Use emollients regularly, especially after bathing, to reduce dryness and scaling.
- Be gentle with your skin. Avoid harsh scrubbing, aggressive exfoliation, and fragranced products if they irritate you.
- Notice your triggers. Stress, illness, and skin injury often matter more than people realise.
- Stick with treatment long enough. Many topical treatments need consistent use before improvement becomes clear.
If your skin is sensitive overall, practical household changes can help reduce irritation. Some people also review their washing products and prefer fragrance-free detergents for eczema, especially when clothing, bedding, or towels seem to aggravate already reactive skin.
The mental side is real
Psoriasis can affect mood, self-esteem, intimacy, and social confidence. Some people avoid swimming, hair appointments, dating, or short-sleeved clothes. Others feel frustrated because friends or relatives minimise it as “just a rash”.
Those reactions are understandable. Psoriasis is visible, recurrent, and sometimes unpredictable. Needing support doesn't mean you're overreacting.
If psoriasis is affecting your confidence or mental health, say so out loud in your appointment. That information is clinically important, not secondary.
Long-term management usually works better than crisis management
A lot of people seek help only when things become unbearable. That makes sense, but it can leave you chasing flares instead of preventing them. Regular review, early adjustment of treatment, and realistic skincare habits often produce steadier control.
What helps most is a plan you can follow. Not a perfect plan. A practical one.
Get Fast, Expert Psoriasis Care with Private Dermatology
When psoriasis is active, waiting can feel like its own problem. If your skin is sore, visible, or affecting sleep and concentration, being told to wait weeks for specialist input can be frustrating.
UK access pressures are real. NHS dermatology waiting times averaged 12 to 15 weeks in 2024 to 2025, with surges to over 20 weeks in some rural areas, according to the evidence cited in this PubMed-listed access summary. For people who need diagnosis, treatment review, or escalation to advanced care, those delays can mean longer discomfort and longer uncertainty.
Why some patients choose private dermatology psoriasis care
Private care isn't only about convenience. For many patients, it's about getting timely answers when symptoms need attention now.
Key benefits often include:
- Rapid specialist assessment so you can find out whether it is psoriasis or another chronic skin condition
- Personalised treatment plans based on the type of psoriasis, body site, and how much it affects daily life
- Review of previous treatments when creams haven't worked or the diagnosis still feels uncertain
- Ongoing follow-up for flare management, treatment adjustment, and longer-term skin health
- Consultant-led care that can be especially useful when symptoms are complex or involve nails, scalp, or possible joint symptoms
When to seek help sooner
You shouldn't wait if:
- Your rash is spreading quickly
- The skin is cracking, painful, or bleeding
- Your scalp or nails are involved
- You have joint pain or stiffness alongside skin symptoms
- You've tried treatment without improvement
- The condition is affecting work, sleep, or confidence
For patients in the UK looking for private dermatology psoriasis support, Haven Medical offers consultant-led care with faster access, individualized assessment, and ongoing management. If you want a specialist opinion without a long delay, you can visit Haven Medical’s website to learn more about available dermatology services.
If persistent skin symptoms are worrying you, click to book a consultation. If you'd prefer to talk first, call to book and discuss what you've been experiencing. If you're comparing options for quicker diagnosis and treatment, visit website pages and choose the service that fits your needs.
This article is for general information only and shouldn't replace personalised medical advice. If you think you may have psoriasis, or if your diagnosed psoriasis is worsening, seek assessment from a qualified healthcare professional.