Some women arrive in clinic convinced they’re “just not coping as well as they used to”. They’re sleeping badly, snapping more easily, losing words mid-sentence, and dragging themselves through the day on caffeine and routine. They often assume it’s stress, work, parenting, poor sleep, or getting older.
Sometimes it is. Often, it’s also perimenopause.
That’s why understanding perimenopause symptoms UK women commonly experience matters so much. The early phase doesn’t always announce itself with obvious hot flushes. For many, the first clues are psychological, neurological, or physical changes that seem unrelated at first glance. Anxiety. Fatigue. Brain fog. Palpitations. A sense that your body has become unfamiliar.
These symptoms and signs of perimenopause are real. They are common. They are also frequently dismissed, including by women who are used to pushing through and by clinicians who only look for the most stereotypical features. A proper assessment should look at the whole picture, not one symptom in isolation.
Feeling ‘Off’? It Might Be More Than Just Stress
A familiar story goes like this. A woman in her early 40s is doing what she’s always done. Managing work, family, deadlines, the invisible household load, and everyone else’s needs. Then things start to shift.
She’s more tired than usual, but not in a simple “I need an early night” way. Her patience is thinner. Small tasks feel mentally heavy. She wakes at 3am and can’t settle again. She forgets names, loses her train of thought, and starts to wonder whether she’s becoming anxious for no clear reason.

In practice, this is one of the commonest ways perimenopause first appears. Not dramatically. Not neatly. Just a growing sense that something is off.
When stress isn’t the full explanation
Stress can absolutely worsen symptoms. Busy lives don’t help. But stress doesn’t explain everything.
If symptoms have become cyclical, unpredictable, or out of character, and especially if they sit alongside changing periods, new sleep problems, low mood, or a drop in resilience, early signs of perimenopause should be on the list of possible causes.
Women often tell me they dismissed the changes for months because they were still having periods. That’s a key reason perimenopause is missed. It starts before periods stop, sometimes years before.
Many women seek help only after months of feeling unlike themselves, because they didn’t realise perimenopause could begin while their cycle was still present.
The hidden pattern
Perimenopause isn’t only about hot flushes. It can show up as:
- Mental strain with anxiety, irritability, or low mood
- Low energy that doesn’t improve properly with rest
- Cognitive changes such as forgetfulness, indecision, or poor concentration
- Sleep disruption even without obvious night sweats
If that sounds familiar, you’re not imagining it. You’re not overreacting. You may be noticing hormonal change, not personal failure.
Understanding Perimenopause and Its Common Signs
Perimenopause is the transition leading up to menopause. In the UK, it typically begins in the mid-40s, although some women notice change earlier and some later. It’s driven by increasingly unpredictable ovarian hormone activity, especially fluctuations in oestrogen and progesterone.
These hormone shifts are not smooth or linear. That’s why symptoms can feel erratic. You may have a month where things are manageable, followed by one where sleep, mood, and physical symptoms suddenly worsen.
What hormones are doing
Oestrogen affects far more than periods. It has effects across the brain, skin, joints, blood vessels, and genitourinary tissues. Progesterone also matters, particularly for sleep, calmness, and cycle regulation.
When these hormones begin to fluctuate rather than follow a reliable pattern, women may notice:
- Cycle changes with periods arriving earlier, later, heavier, lighter, or becoming less predictable
- Temperature symptoms such as hot flushes and night sweats
- Mood and energy changes that don’t feel typical for them
- Physical shifts affecting sleep, libido, and body comfort
Large-scale symptom data shows that in perimenopause, hot flushes affect 83.4% of women and fatigue affects 74.8%, highlighting that both the classic and more general symptoms are common in this phase, as outlined in this large-scale analysis of perimenopause symptom patterns.
The signs most people already know
Most women have heard of a few hallmark symptoms. These include:
- Irregular periods
- Hot flushes
- Night sweats
- Vaginal dryness
- Changes in libido
If you want a patient-friendly overview, this detailed guide to the 34 symptoms of perimenopause is a useful starting point.
Why the symptom pattern feels confusing
Perimenopause doesn’t behave tidily. Symptoms can:
| Pattern | What that can look like |
|---|---|
| Come and go | A difficult month followed by a quieter one |
| Shift over time | Anxiety first, then sleep disruption, then flushes |
| Overlap with other issues | Stress, thyroid problems, burnout, low iron, poor sleep hygiene |
| Feel disproportionate | A level of exhaustion or mental fog that seems out of keeping with life circumstances |
That’s why many women spend a long time trying to explain separate symptoms, rather than seeing one hormonal thread connecting them.
The Unexpected Perimenopause Symptoms You Should Not Ignore
A woman may come to clinic convinced she is burning out. She is more anxious than usual, forgetting words in meetings, sleeping badly, and snapping at people she loves. Her periods may still be coming, so perimenopause is not on her list. In practice, this pattern is common.
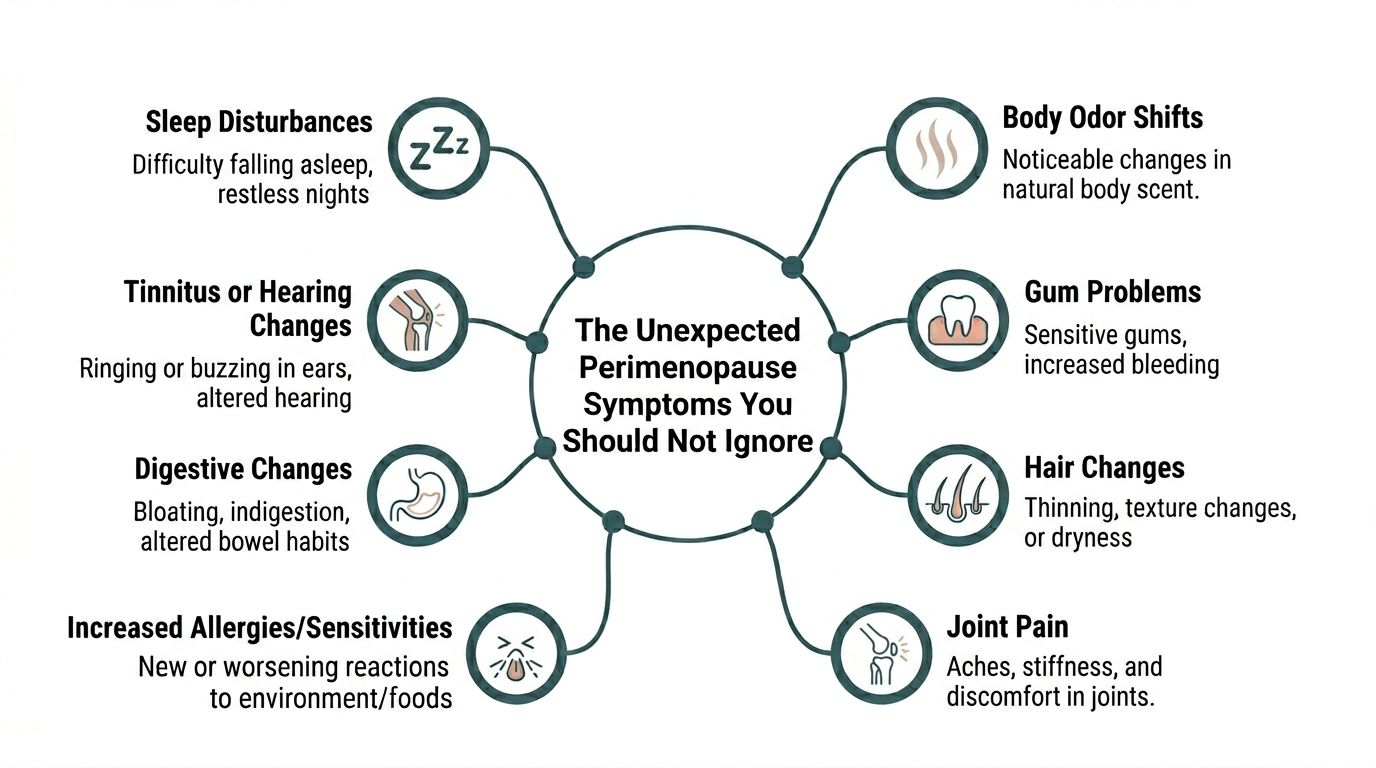
The symptoms that unsettle women most are often not the ones they were warned about. Hot flushes matter, but they are not always the opening sign. For many women in the UK, the first clues are psychological and neurological. Anxiety. Poor concentration. Brain fog. A sense of feeling unlike yourself.
Fatigue that feels out of proportion
Perimenopausal fatigue often feels heavier than ordinary tiredness. Women describe waking unrefreshed, losing stamina halfway through the day, or feeling as if rest no longer restores them properly.
Sleep disruption is often part of it, but not all of it. Hormonal fluctuation can affect sleep quality, stress tolerance, and day-to-day recovery. A useful clinical clue is the gap between what your life demands and how depleted you feel. If the exhaustion seems out of keeping with your workload, health, or usual resilience, it should be assessed properly.
Anxiety, low mood, and sudden panic symptoms
This is one of the most commonly dismissed presentations. A woman in her 40s develops anxiety out of nowhere, starts waking with a racing heart, or feels persistently on edge, and the assumption is often stress, overwork, or a primary mental health problem.
Sometimes those explanations are right. Sometimes they are incomplete.
Psychological symptoms can be an early sign of perimenopause, particularly when they appear alongside sleep change, cycle shifts, irritability, or problems with focus. In clinic, I take new anxiety in midlife seriously because it deserves a wider lens. The aim is not to label every mood change as hormonal. The aim is to stop missing a hormonal contribution when the pattern fits.
Clinical reality: If anxiety is new, worse than usual, or paired with brain fog, poor sleep, or period changes, perimenopause belongs on the differential diagnosis.
Brain fog and memory lapses
Brain fog is not a throwaway phrase. Women use it because it describes a recognisable change. Word-finding becomes slower. Concentration becomes effortful. Multitasking, which once felt manageable, suddenly feels chaotic.
This can be professionally and emotionally unsettling, especially for women in demanding jobs or caring roles. Some worry they are becoming less capable. Others fear something more serious.
There are many possible contributors to cognitive symptoms, including sleep loss, anxiety, ADHD, thyroid problems, low iron, medication effects, and depression. Perimenopause is one of them, and it is often missed when hot flushes are absent. That matters, because reassurance alone is not enough. Women need a proper assessment of the full picture.
Sleep problems, even without obvious night sweats
Poor sleep is one of the most disruptive symptoms in this phase. Some women struggle to fall asleep. Others wake at 3am and cannot settle again. Some sleep for enough hours on paper but still wake feeling exhausted.
Night sweats can cause this, but they are not the only mechanism. Hormonal shifts can affect sleep quality directly, and anxiety often makes the problem worse. The result is a loop. Sleep deteriorates, mood worsens, concentration drops, and daily life becomes harder to manage.
That loop is one reason perimenopause is sometimes mistaken for burnout.
Joint aches and muscle discomfort
Aching hands, stiff hips, sore shoulders, or a general sense of muscular heaviness can all show up in perimenopause. Many women put it down to age, exercise strain, bad posture, or the mattress. Those factors can play a part, but they are not the whole story.
Fluctuating oestrogen can affect pain sensitivity, inflammation, and tissue comfort. Symptoms often feel worse after poor sleep or at certain points in the cycle. This does not mean every ache is hormonal. It means joint and muscle symptoms deserve to be considered alongside the rest of the pattern.
Skin and hair changes
Skin and hair often reflect hormonal change earlier than expected. Women may notice drier skin, increased sensitivity, slower healing, hair thinning, or a change in hair texture.
These symptoms are easy to dismiss as cosmetic, but they can be clinically useful when they appear alongside mood change, sleep disruption, and cycle irregularity. Timing matters. Clustering matters.
Reduced libido
Low libido is common and often left unspoken. Desire can fall because of hormonal shifts, but it is rarely one-dimensional. Fatigue, poor sleep, vaginal dryness, anxiety, body image concerns, and relationship strain can all contribute at the same time.
That is why a good assessment looks beyond one symptom. If sleep improves, vaginal symptoms are treated, or anxiety is better controlled, libido often improves as well.
Heart palpitations
Palpitations can feel alarming. Some women notice fluttering, pounding, missed beats, or a sudden awareness of their heartbeat, especially at night or during anxious spells.
Perimenopause can be part of the explanation, but it should not be used as a shortcut diagnosis. Palpitations can also relate to caffeine, thyroid disease, anaemia, heart rhythm problems, medication, or panic symptoms.
If palpitations are frequent, worsening, or linked with chest pain, breathlessness, dizziness, or fainting, they need medical review.
Weight changes and altered metabolism
Weight change in midlife is rarely simple. Some women gain weight. Others notice more abdominal fat, bloating, or a body composition shift despite keeping the same habits.
Hormonal fluctuation may contribute, but sleep loss, lower activity from fatigue or joint pain, stress, medication, alcohol, and thyroid or metabolic issues all need consideration. Blaming weight changes on willpower helps no one. The useful question is what has changed in the background.
A quick symptom map
| Symptom | Why it’s commonly missed |
|---|---|
| Fatigue | Blamed on work, parenting, poor sleep, or low iron |
| Anxiety | Treated as stress alone or a stand-alone mental health issue |
| Brain fog | Put down to overload, burnout, or ageing |
| Sleep disruption | Managed as insomnia without asking about hormones |
| Joint pain | Assumed to be exercise strain, arthritis, or posture |
| Hair and skin changes | Viewed as cosmetic rather than part of a hormonal pattern |
| Reduced libido | Normalised, avoided, or disconnected from other symptoms |
| Palpitations | Attributed only to anxiety |
| Weight change | Reduced to lifestyle or self-control |
The pattern matters more than any single symptom in isolation. When anxiety, brain fog, sleep disruption, physical discomfort, and cycle changes start clustering together, perimenopause should be considered early, not as an afterthought.
Why Early Perimenopause Symptoms Are So Often Missed
A woman in her early forties comes in saying she no longer feels like herself. She is more anxious than usual, her concentration has slipped, she wakes at 3am for no clear reason, and small tasks feel oddly hard to finish. Her periods are still coming, perhaps a little closer together or slightly heavier, so perimenopause has not crossed her mind. In many cases, it has not crossed anyone else’s either.
That is one of the main reasons early perimenopause is missed. The first signs are often psychological or neurological rather than the symptoms people expect. In UK practice, I often see women referred for anxiety, burnout, poor sleep, or possible ADHD relapse before anyone has asked whether these changes follow a hormonal pattern.
Symptom overlap can blur the diagnosis
Early perimenopause sits in uncomfortable diagnostic territory. Anxiety, low mood, palpitations, fatigue, and poor concentration are common symptoms in general practice, and they have several possible causes. Thyroid disease, anaemia, medication side effects, depression, sleep apnoea, alcohol use, and cardiovascular problems may all need to be considered.
Good clinicians should think widely. The problem comes when hormone change is left out of that wider assessment, especially if hot flushes are absent.
Many women do not present by saying, "I think this is perimenopause."" They present with a cluster of issues that has built up over months. A prescription for sleep, a discussion about stress, or separate referrals for mood and palpitations can each seem reasonable in isolation. The pattern can still be missed.
Hormonal fluctuation rarely produces a neat timeline
Perimenopause is inconsistent by nature. Symptoms can flare for two weeks, settle for a month, then return in a different form. Brain fog may be prominent one cycle. Anxiety or insomnia may dominate the next. Some women feel noticeably worse in the days before a period, then improve enough to doubt their own account.
That stop-start pattern affects diagnosis. It also affects confidence. Many women arrive apologising for "making a fuss" because the symptoms are not constant, even though the overall trend is clear once the history is taken properly.
A single appointment can miss that story.
Many women have been trained to explain it away
There is also a social reason these symptoms are overlooked. Midlife women are often carrying work pressure, family care, poor sleep, and the expectation that they should cope without complaint. If they become tearful, forgetful, overwhelmed, or short-tempered, they are often told they are stressed, doing too much, or getting older.
Sometimes stress is part of the picture. Often it is. But stress and perimenopause are not mutually exclusive, and treating one while ignoring the other usually leaves women feeling unheard.
Many women do not minimise their symptoms because they are mild. They minimise them because they have spent years being told to push through.
The hot flush stereotype still gets in the way
Public understanding of perimenopause is still too narrow. Many women expect the first sign to be flushes, night sweats, or obvious cycle disruption. If those are not present yet, they may rule perimenopause out themselves. Some clinicians do the same.
That is where early cases are lost. Anxiety that appears out of character, new cognitive difficulties, disrupted sleep, sensory overwhelm, reduced resilience, and a sense of being mentally unlike oneself can all be early features of perimenopause. They deserve to be taken seriously, particularly when they appear together or alongside even subtle menstrual change.
The question is not whether every woman with brain fog or anxiety is perimenopausal. The question is whether the possibility has been considered early enough, and in the right clinical context.
The Importance of a Clinically Guided Assessment
A woman in her early forties comes in convinced she is burning out. She feels wired at night, anxious for no clear reason, forgetful in meetings, and unlike herself with her family. Her periods are still coming, so perimenopause has not seemed like the obvious explanation. That kind of history is common, and it is exactly why assessment needs to be clinical rather than assumptive.

Diagnosis is about patterns, not guesswork
Perimenopause is usually identified by the overall pattern. Age matters, but so do cycle changes, sleep disruption, anxiety, cognitive symptoms, physical changes, medical history, contraception, and the timing of everything together.
In practice, the psychological and neurological symptoms often need the closest attention. New anxiety, a shorter emotional fuse, poor concentration, sensory overload, and brain fog can all appear before hot flushes become obvious. In the UK, those symptoms are still too often separated from hormonal assessment and treated as stress alone. A good consultation puts them back into context.
That matters because the question is rarely, "Is this hormones or mental health?" It is often both, interacting at the same time.
Where blood tests help, and where they don’t
Many women ask for a blood test to confirm perimenopause. Sometimes tests are useful. Just not in the simplistic way people are often led to expect.
Hormone levels can fluctuate significantly during perimenopause, so a single result may not reflect what is happening across the month. For many women over 45 with a typical history, diagnosis is clinical. Tests become more helpful when the picture is less clear, when symptoms start earlier than expected, or when another condition could be contributing.
I often use blood tests to check for things that can mimic or worsen perimenopausal symptoms, such as thyroid disease, anaemia, low iron, low B12, or vitamin D deficiency. That can prevent two common mistakes. Missing a treatable medical problem, or blaming every symptom on hormones.
What a useful assessment should cover
A useful review should look at more than one symptom in isolation. It usually includes:
- Cycle history, including timing, flow, skipped periods, and subtle pattern change
- Symptom mapping across mood, sleep, concentration, memory, physical symptoms, and sexual health
- Medical risk review including migraine history, blood pressure, clot risk, and family history where relevant
- Medication and contraception review
- Mental health assessment to distinguish longstanding anxiety or depression from a new hormone-linked change, while recognising they may overlap
Good menopause care does not depend on one lab result. It depends on listening carefully, spotting patterns, and ruling out what should not be missed.
Why self-diagnosis has limits
Many women are right to suspect perimenopause before they speak to a clinician. That instinct is often sound.
The limitation is context. Anxiety and brain fog may fit perimenopause, but they can also occur with thyroid problems, sleep apnoea, iron deficiency, medication effects, depression, ADHD, or prolonged stress. The opposite problem happens too. Women with clear perimenopausal symptoms are told they are stressed because they are still having periods or are considered "too young".
A clinically guided assessment reduces both risks. It gives a clearer diagnosis, a safer treatment plan, and, equally important, the relief of having the full picture taken seriously.
Your Path to Clarity and Relief with Haven Medical
When women seek help from a private menopause clinic UK service, what they usually want isn’t only treatment. They want clarity. They want someone to take the full symptom picture seriously and explain what’s happening.
At Haven Medical, that process starts with a GP-led, clinician-led assessment rather than a rushed conversation focused on one complaint. That matters because perimenopause often affects several areas at once. Mood, sleep, periods, cognition, libido, pain, and confidence in daily functioning can all be part of the same story.
What guided care looks like in practice
A thoughtful plan usually includes three parts.
First, a proper review of symptoms and timing. That means looking at patterns, not isolated events.
Second, broader health assessment where needed. Some women need hormone-focused discussion. Some also need checks for other causes of fatigue, palpitations, mood change, or sleep disruption.
Third, an individualised management plan. There is no single best treatment for every woman.
What tends to work best
For vasomotor symptoms affecting 80% of UK perimenopausal women, NICE-supported low-dose HRT can reduce frequency by 70-80%. For mood and sleep disruption, evidence-based approaches such as CBT can achieve a 40% symptom reduction.
Those figures matter because they show a guided treatment plan can help meaningfully. They also show why one-size-fits-all advice often falls short.
In practice, treatment may involve:
- Hormonal treatment where appropriate and safe
- Non-hormonal strategies for women who can’t or don’t want to use hormones
- CBT-based support for sleep, anxiety, and coping patterns
- Lifestyle adjustments targeted at symptom triggers, rather than vague advice to “be healthier”
- Follow-up and monitoring so treatment can be adjusted rather than abandoned
What doesn’t work well
Most women have already tried the obvious things before seeking care. Sleeping earlier, cutting back caffeine, buying supplements at random, and telling themselves to push through.
Sometimes those help a little. They rarely solve the bigger picture on their own when hormones are playing a significant role.
Haven Medical offers the sort of joined-up care many women struggle to access elsewhere, with private GP support and access to wider consultant-led services when needed. If your symptoms sound familiar, call to book, click to book, or visit website to arrange a confidential consultation.
Conclusion Taking Control of Your Perimenopause Journey
If you’ve been feeling flat, anxious, foggy, restless, short-tempered, achy, or unlike yourself, don’t dismiss it because it doesn’t fit the stereotype. Perimenopause can begin subtly, and its symptoms can look much broader than most women are ever told.
The important step is not guessing perfectly. It’s recognising that your symptoms are valid and worthy of proper assessment.
You don’t need to put up with feeling unwell while wondering if it’s stress, burnout, age, or something else entirely. Support is available, and treatment can be individualized. If you’re also exploring self-care options, this guide to best supplements for menopause may help you think more carefully about what’s worth discussing with a clinician rather than buying blindly.
A good consultation should leave you with a clearer explanation, safer options, and a plan that fits your life. If you recognise yourself in these symptoms and signs of perimenopause, Haven Medical can help you move from uncertainty to informed, supported care.
If you’re ready to stop second-guessing what your body is telling you, book a confidential appointment with Haven Medical. The right assessment can make the whole picture make sense.
Frequently Asked Questions
Can perimenopause start in your 30s
It can, but most women in the UK begin to notice perimenopause in the mid-40s. If you’re in your 30s with symptoms that sound hormonal, don’t assume and don’t ignore them. Get assessed properly so other causes aren’t missed.
Do I need a blood test to diagnose perimenopause
Not always. Diagnosis is often based on symptoms, cycle changes, and your wider clinical history. Blood tests can be helpful in some situations, especially when symptoms overlap with other conditions, but they’re not a perfect standalone answer.
Can perimenopause cause anxiety without hot flushes
Yes. Anxiety can be an early feature, and for some women it appears before the more widely recognised vasomotor symptoms. That’s one reason perimenopause is often overlooked.
What are the most overlooked perimenopause symptoms UK women report
Commonly missed symptoms include fatigue, sleep disruption, brain fog, anxiety, joint aches, reduced libido, and palpitations. They are often misattributed to stress, ageing, or lifestyle.
Is HRT the only treatment option
No. Some women do very well with hormone treatment. Others need a non-hormonal approach, or a combination of options such as CBT, symptom tracking, sleep support, and targeted lifestyle changes. Treatment should be individual.
How do I talk to my employer about symptoms
Keep it practical. Explain the symptoms affecting your work, such as sleep disruption, concentration problems, or anxiety, and ask for adjustments that would help. That might mean flexibility, a cooler environment, regular breaks, or support during difficult phases. A clear medical assessment can make those conversations easier.