If you’re reading this after another painful feed, you’re not alone. Many parents arrive at the same point. Their baby seems hungry but can’t stay latched well, feeds take a long time, there’s clicking, slipping off the breast, wind, frustration, and sore nipples that make the next feed feel daunting.
That can leave you wondering whether you’re doing something wrong. In many cases, you aren’t. One possible reason is tongue-tie, also called ankyloglossia. When tongue movement is restricted, feeding can become much harder work for both baby and parent.
The good news is that tongue-tie is common, it can be assessed properly, and when it is causing symptoms, treatment can help. If you’re searching for tongue tie treatment UK, the most important first step isn’t rushing into a procedure. It’s understanding what tongue-tie is, how it affects function, and when expert treatment is the right answer.
Understanding Tongue-Tie and Its Signs in Your Baby

A tongue-tie happens when the lingual frenulum, the small band of tissue under the tongue, is tight or short enough to limit how freely the tongue moves. In simple terms, the tongue can’t lift, extend, or shape itself as well as it needs to.
That matters because the tongue does more than sit in the mouth. In a baby, it helps create an effective seal, maintain suction, and draw milk efficiently during feeding. In older children and adults, it also contributes to speech and oral function.
What tongue-tie can look like in real life
Some babies with tongue-tie have no problems at all. In the UK, with over 680,000 live births each year, around 60,000 babies are affected, with reported prevalence ranging from 4% to 11%, and 75% of infants with tongue-tie remain asymptomatic and have no feeding problems, according to this UK review of ankyloglossia.
That point is reassuring and important. A visible frenulum does not automatically mean a baby needs treatment.
When tongue-tie is causing trouble, parents often notice patterns such as:
- Difficulty latching well. Baby seems to struggle to stay attached or slips off the breast.
- Clicking during feeds. This can suggest loss of suction.
- Very long or very frequent feeds. Baby may be working hard but not feeding efficiently.
- Nipple pain for the mother. A shallow latch can cause significant discomfort.
- Frustration at the breast or bottle. Baby may pull away, cry, or seem unsettled.
- Wind after feeding. Taking in more air can make babies uncomfortable.
Some parents also notice that the tongue doesn’t seem to move forward easily, or that the tongue tip looks notched or heart-shaped when the baby cries.
When parents get confused
The hardest part is that tongue tie in babies doesn’t always look dramatic. A baby can appear to latch, and yet feeding still isn’t going well. That’s why function matters more than appearance alone.
Practical rule: If feeding is painful, prolonged, or consistently stressful, it’s worth having both feeding technique and tongue function assessed.
Parents often feel relief from having the problem named. Once you understand the mechanics, the situation becomes less mysterious and much more manageable.
How Tongue-Tie Disrupts Feeding for Mother and Baby
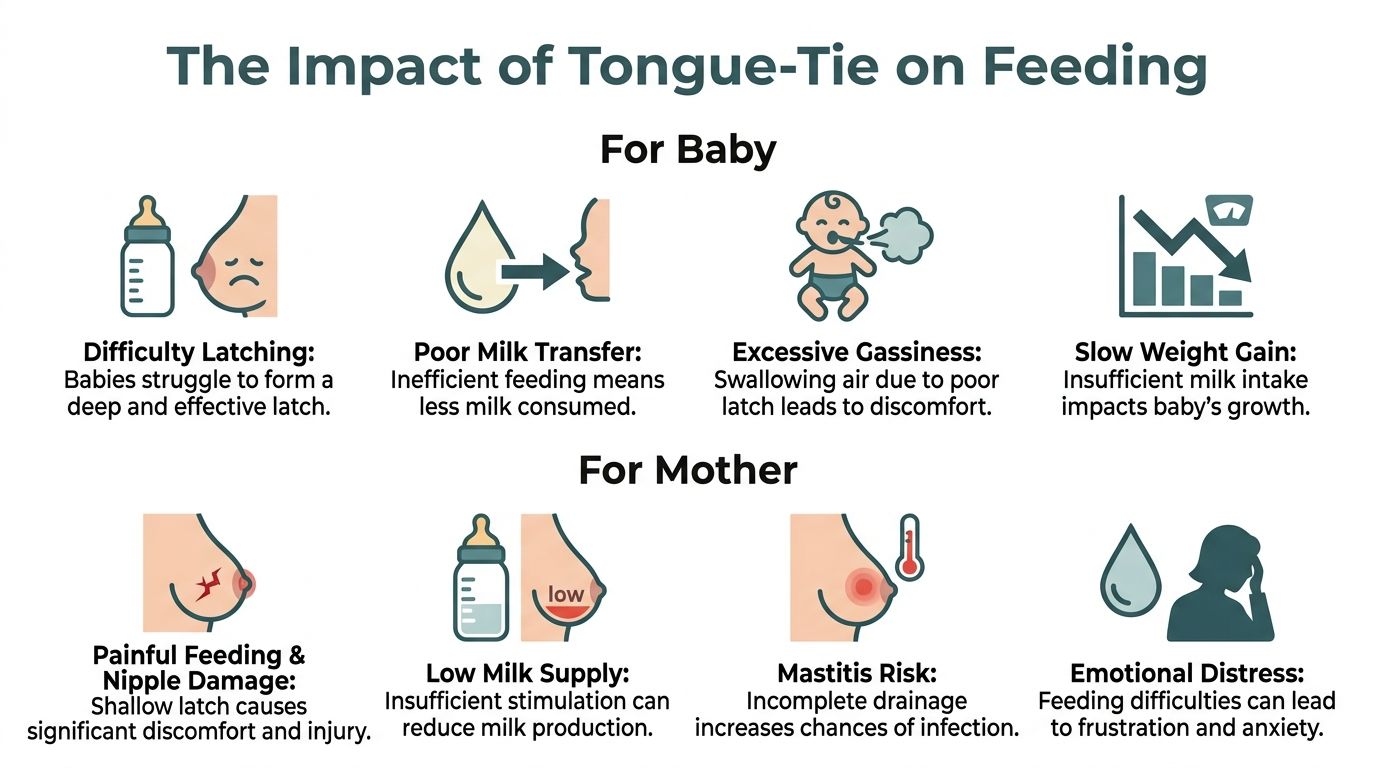
Feeding difficulties from tongue-tie are usually mechanical. The problem isn’t lack of effort. It’s that the tongue can’t move with the range and coordination needed for an efficient feed.
Why latch becomes ineffective
For breastfeeding to work well, a baby needs to take a deep mouthful of breast tissue and use the tongue to cup, lift, and maintain suction. If tongue movement is restricted, the latch often becomes shallow.
A shallow latch changes everything. Baby may compress the nipple instead of feeding effectively, lose suction, swallow more air, and come off repeatedly.
That can lead to a familiar pattern:
| Feeding issue | What parents may notice |
|---|---|
| Poor latch | Slipping off, repeated relatching, clicking |
| Inefficient milk transfer | Long feeds, hunger soon after feeds, frustration |
| Extra air intake | Wind, gassiness, unsettled behaviour |
| Fatigue at feeds | Baby dozes off, then wakes hungry again |
This is why breastfeeding tongue tie can feel so exhausting. The feed may be constant, but the milk transfer may still be poor.
Why mothers often feel the impact so strongly
A restricted tongue doesn’t just affect the baby. It can make feeding physically painful for the mother.
When baby can’t maintain a deep latch, the nipple may be pinched, rubbed, or compressed. Over time that can lead to soreness, visible trauma, dread before feeds, and loss of confidence. Some mothers also worry that their milk supply is falling because feeds are so inefficient.
Pain during feeding isn’t something you should push through if it persists. Ongoing pain is a sign that feeding needs a proper review.
Bottle-fed babies can also struggle. They may dribble milk, gulp, click, tire quickly, or take in excess air. So while tongue-tie is often discussed in relation to breastfeeding, baby feeding difficulties tongue tie can involve either breast or bottle feeding.
The emotional toll is real
When feeding hurts or never seems to satisfy the baby, parents often feel guilt, anxiety, and confusion. They may try different positions, shields, bottles, and schedules without knowing that tongue restriction could be contributing.
Support from a feeding specialist can make a big difference. This article on working with a Tongue Tie Lactation Consultant gives a useful overview of how feeding assessment and tongue-tie evaluation can work together.
For symptomatic babies, there is evidence that treatment can help quickly. A UK-relevant study found that 95% of infants with tongue-tie and feeding difficulties who underwent frenotomy showed breastfeeding improvement within 48 hours, compared with 5% in untreated controls, as reported in the Infant journal review.
That doesn’t mean every feeding problem is caused by tongue-tie, and it doesn’t mean every visible tie should be divided. It does mean that in the right baby, with the right symptoms, treatment may change feeding remarkably fast.
The Frenulotomy Procedure What to Expect at Haven Medical
For many parents, the word “procedure” is the part that causes the most worry. That’s understandable. When the patient is your baby, even a minor treatment can feel emotionally huge.
In practice, a frenulotomy consultation should feel calm, careful, and unhurried. The aim is to make sure treatment is appropriate, explain the options clearly, and support feeding afterwards. At Haven Medical, we are very lucky to have Mrs Kate Heathcote, an ENT Consultant, carry out our tongue tie procedures; with years of experience, Kate is an expert in this area.
Before treatment
The first part is assessment. A clinician doesn’t just look under the tongue and make a snap decision. They ask about feeding, symptoms, weight concerns, nipple pain, and what you’ve already tried.
They also examine how the tongue moves. The key question is not, “Can I see a frenulum?” It’s, “Is this frenulum restricting function enough to explain the symptoms?”
If treatment is recommended, the clinician explains:
- Why treatment is being considered
- What the procedure involves
- What discomfort or bleeding may occur
- What feeding may look like afterwards
- What aftercare is advised
That discussion matters. Good care is never rushed.
During the procedure
In a young baby, frenulotomy is usually a quick division of the restrictive tissue under the tongue. It is commonly performed without general anaesthetic.
Parents often want to know what “quick” really means. In many infant cases, it takes only moments. The baby is held securely, the tongue is lifted, and the clinician divides the tight frenulum with an appropriate instrument.
There may be a small amount of bleeding. That’s usually limited and brief. Babies are often encouraged to feed soon afterwards, which can be both comforting and practical.
The experience is usually harder for the parent watching than for the baby having the procedure.
For thicker or more complex frenula, older children, or adults, the approach may differ. The Mayo Clinic treatment summary notes that Royal College of Surgeons benchmarks describe 95% mobility restoration with frenuloplasty for thick frenula, compared with 85% for scissor frenotomy in infants under six months, and that post-operative exercises can reduce reattachment by 80%.
After treatment
Recovery is usually straightforward, but aftercare still matters. You may be shown feeding positions, wound care advice, and exercises if they are appropriate for the age and procedure type.
Common questions after treatment include:
- Will baby feed normally straight away? Some do. Others need a short adjustment period.
- Will there be soreness? There can be temporary tenderness.
- Do we need follow-up? Good practice usually includes review, especially if feeding issues were significant before treatment.
The Immediate Benefits of Tongue-Tie Treatment
What may improve for baby
Once tongue movement is freer, the latch may become deeper and more stable. Milk transfer may improve. Feeds may become calmer and less frantic.
Parents commonly hope for improvements such as:
- A stronger latch with less slipping on and off
- More effective feeds rather than constant snacking
- Less swallowing of air, which may reduce wind and discomfort
- A more settled baby after feeding
- Better overall nourishment when feeding becomes efficient
These changes matter because feeding isn’t only about calories. It’s also about comfort, rhythm, and helping baby feel satisfied.
What may improve for mother
For many mothers, the most meaningful change is pain relief. If nipple pain has been severe, reducing that discomfort can be a significant improvement.
Other likely benefits include:
| For mother | Why it matters |
|---|---|
| Less nipple pain | Feeding becomes more sustainable |
| Better confidence | Parents stop blaming themselves |
| Shorter feeds | More time to rest and recover |
| Less stress around feeding | Bonding becomes easier |
This is why tongue tie treatment UK isn't only about the baby's mouth. It can also protect a mother's physical comfort and emotional wellbeing during a demanding stage of life.
Relief doesn't always mean perfection on day one. Sometimes the improvement is immediate. Sometimes feeding gets better over several days as baby relearns how to use the tongue more effectively.
That distinction is helpful. A successful procedure can open the door to better function, but some babies still need time, positioning support, or lactation input to get the full benefit.
Why quick wins matter so much
Early feeding problems can affect the whole household. Every painful latch, every unsettled evening, every extra hour spent trying to feed adds pressure.
When treatment helps, the result is often bigger than the procedure itself. Parents can begin to enjoy feeding again. Baby may seem calmer. The home atmosphere often becomes less tense.
Those early improvements are the reason many families seek help. Not because they want unnecessary intervention, but because they want feeding to become comfortable, effective, and emotionally manageable.
Long-Term Improvements for Speech and Oral Health
Feeding is usually the first concern, but tongue movement also matters later in childhood and adulthood. The tongue helps with speech, swallowing, oral clearance, and the resting posture of the mouth.
Speech and clear tongue movement
A tongue that can't lift or extend well may affect articulation of certain sounds. According to the Hopkins tongue-tie overview, untreated tongue-tie is linked to a 15% to 20% higher risk of Class III malocclusion due to low tongue posture. The same source notes that tongue restriction can impair articulation of sibilants such as s, z, th and linguals such as t, d, n, l, with assessments showing restricted protrusion of less than 2 mm beyond the lower vermillion border or poor elevation to the palate.
That doesn't mean every child with unclear speech has a tongue-tie, or that every tongue-tie will cause a speech problem. It means tongue mobility is one factor worth assessing when speech sounds are persistently difficult.
Oral function in daily life
Older children and adults may describe more mechanical problems than speech problems. Common examples include:
- Difficulty licking food from the lips
- Trouble moving food around the mouth
- Problems clearing food debris from teeth
- A sense of tension under the tongue
- Awkward tongue movements during eating or oral hygiene
These issues can be subtle. Some people adapt so well that they don't realise their tongue movement is limited until they're assessed.
Why adults sometimes seek treatment
Adults with untreated tongue-tie often say they have "always managed", but still feel restricted. They may notice speech effort, oral discomfort, or frustration with tongue movements that others find easy.
Treatment in older children and adults needs individual assessment. The procedure may be different from an infant frenulotomy, and aftercare is often more important because habits and compensation patterns are more established.
The key point is simple. Tongue-tie isn't only a newborn issue. When it affects function later in life, careful assessment can help clarify whether treatment is likely to improve comfort, movement, or speech support.
Why Expert Medical Assessment is Crucial
Tongue-tie is one of those conditions that can be both under-recognised and over-called. That's exactly why a proper medical assessment matters.
Some babies have a visible frenulum and feed perfectly well. Others have a less obvious restriction but clear functional problems. Looking alone isn't enough.
Function matters more than appearance
A responsible assessment focuses on questions such as:
- Is the tongue moving freely enough for feeding?
- Do the symptoms fit the restriction seen on examination?
- Have other feeding factors been considered?
- Would conservative support help first, or is treatment appropriate now?
This protects families in both directions. It helps avoid missing a clinically important tongue-tie, and it helps avoid unnecessary procedures when the frenulum isn't the true cause of the problem.
Why caution is good medicine
There are rising concerns about overdiagnosis and increasing frenotomy rates without strong evidence for long-term efficacy. A discussion of overdiagnosis and assessment-first care notes that Cochrane Reviews show limited infant feeding improvements despite maternal pain relief, and that the NHS emphasizes frenotomy only for symptomatic cases.
That can sound confusing to parents. If some studies show rapid feeding improvement, why the caution?
The answer is that both points can be true. Some babies clearly benefit, especially when symptoms and tongue restriction match well. At the same time, not every feeding difficulty is caused by tongue-tie, and not every visible tie needs division.
Good clinicians don't ask, "Can I cut this?" They ask, "Will this help this particular patient?"
What a high-quality assessment should include
A strong assessment usually brings together several strands of information:
| Part of assessment | Why it matters |
|---|---|
| Feeding history | Shows the practical impact on baby and parent |
| Examination of tongue movement | Identifies whether function is restricted |
| Review of latch or bottle feeding | Helps separate tongue issues from positioning or flow issues |
| Discussion of alternatives | Prevents procedure-first thinking |
| Clear aftercare planning | Supports better recovery and feeding adjustment |
This balanced approach is especially important when parents are anxious and looking for quick answers online. The goal should never be to dismiss concerns, but to answer them carefully and openly.
Your Path to Comfortable Feeding Starts at Haven Medical
If feeding has become painful, stressful, or exhausting, getting help is a positive step. Tongue-tie is common, often manageable, and when treatment is appropriate, it can make a meaningful difference to comfort and function.
What matters most is the standard of care around the decision. Families deserve assessment-led advice, clear explanations, and support after treatment. They also deserve honesty if a procedure isn't needed.
At Haven Medical, care is clinician-led, family-centred, and designed to support babies, children, and adults with thoughtful assessment and treatment where appropriate. As a private tongue tie clinic within a broader medical setting, Haven Medical offers access to consultant-led care, day surgery support, and a team that understands how feeding concerns affect the whole family.
If the signs in this guide sound familiar, you don't need to keep guessing.
- Call to book a consultation if your baby has ongoing latch problems, painful feeds, or suspected tongue-tie.
- Click to book an appointment and get a proper assessment of tongue function and feeding concerns.
- Visit website to learn more about Haven Medical's clinician-led services at thehavenmedical.com.
A calm, expert review can bring clarity quickly. For many families, that's the moment things start to feel easier.
Frequently Asked Questions About Tongue-Tie Treatment
Does every tongue-tie need treatment
No. Some tongue-ties don't cause any symptoms at all. Earlier in the article, we covered that many babies with tongue-tie are asymptomatic. Treatment is usually considered when there is a clear functional problem, such as feeding difficulty, pain, or later mechanical issues.
The decision should be based on what the tongue can and can't do, not only on how the frenulum looks.
Is tongue-tie always the reason for feeding problems
No. Feeding can be affected by latch technique, positioning, milk flow, prematurity, oral coordination, maternal discomfort, and other factors.
That's why an assessment should look at the whole feeding picture. A visible tongue-tie can be present without being the main cause.
Is the procedure painful for babies
Parents often expect the worst, but infant frenulotomy is usually brief and commonly tolerated well. Babies may cry because they are being held still, because the mouth is being examined, or because the experience is unfamiliar.
Some babies feed almost immediately afterwards. Others are unsettled for a short period. Good preparation and calm aftercare make a difference.
Can tongue-tie affect bottle feeding too
Yes. A baby doesn't need to breastfeed for tongue-tie to matter. Restricted tongue movement can still interfere with seal, suction, pacing, and comfort during bottle feeding.
Parents may notice dribbling, clicking, swallowing air, frequent pauses, or tiring part way through a bottle.
What is posterior tongue-tie
Posterior tongue-tie is a term used when restriction is thought to come from tissue that is less obvious on simple inspection, sometimes under the mucosal surface rather than as a clearly visible front tie.
Emerging concerns over posterior tongue-tie are increasing in the UK, yet public NHS resources often don't address it fully. The Balanced Dental discussion of posterior tongue-tie concerns also notes that the Academy of Breastfeeding Medicine rejects routine lip and cheek tie surgery because of limited evidence, which is why careful assessment of tongue function itself is so important.
That means posterior tongue-tie shouldn't be diagnosed casually. It requires experienced clinical examination, especially when symptoms are significant but the anatomy isn't obvious.
Should lip-tie or cheek-tie always be treated too
Not automatically. Lip and cheek ties are often discussed online alongside tongue-tie, but they are not the same thing, and they don't carry the same evidence base for treatment.
A clinician should decide whether any tissue restriction is affecting function. Procedure-first thinking is not good care.
Can tongue-tie grow back after treatment
The exact concern is usually reattachment, not the body "growing a new tie". Healing tissue can tighten again if the wound closes in a way that reduces movement.
That's one reason aftercare matters. Depending on the age of the patient and the type of procedure, clinicians may advise review, feeding support, or specific exercises.
How quickly will feeding improve
Some families notice a change at the very next feed. Others see a more gradual improvement over days as the baby relearns tongue movement and parents adjust latch or bottle technique.
If feeding remains difficult after treatment, it doesn't always mean the procedure failed. It may mean more feeding support is needed.
Can older children and adults still benefit from treatment
Yes, in some cases. Older children may be assessed for speech concerns, oral function, or mechanical restriction. Adults sometimes seek help for tension, speech effort, or longstanding difficulty with tongue movements.
The treatment plan is usually more individual at those ages. Some need a simple release, while others need a more involved approach and structured aftercare.
How do I know whether to book an assessment
Book an assessment if feeding is painful, your baby can't maintain a good latch, feeds are persistently difficult, or you suspect tongue restriction is affecting speech or oral function in an older child or adult.
You don't need to decide on treatment before seeking help. You only need a proper evaluation from someone who understands both the anatomy and the everyday symptoms.