If you’re reading about weight loss injections UK options, there’s a good chance you’ve already done the exhausting part. You’ve tried to eat better, tried to be more active, and tried to stay consistent. You may even have lost weight before, only to watch it return despite real effort.
That pattern doesn’t mean you’ve failed. It usually means weight regulation is more medically complex than often acknowledged.
Weight loss by injection has changed the conversation because these medicines can help reduce hunger, improve fullness, and make meaningful weight loss more achievable for the right patient. But there is a major difference between obtaining an injection and receiving proper treatment. These are not beauty products, and they are not harmless shortcuts. They are prescription medicines with real benefits, real side effects, and real consequences if they are used badly.
In private practice, the most important question isn’t ‘Which injection will see the greatest weight loss?’ It’s “How do we use this safely, sensibly, and in a way that protects your long-term health?”
The New Era of Weight Management in the UK
Weight-loss medicines have become prominent for a clear reason. Many patients have spent years doing what they were told should work, then feeling blamed when it didn’t last. For some, weight loss by injection is the first treatment that feels biologically aligned with the problem.

Why demand has surged
Public interest has grown faster than the healthcare system has adapted. In the UK, access through standard routes is limited for many people, even when weight is affecting blood pressure, mobility, sleep, confidence, or metabolic health.
A recent discussion of UK access inequalities notes that NHS approvals are limited to specific BMI criteria, often BMI ≥35 with comorbidities, and that many people therefore turn to private care costing £170-£250 per month, creating a “two-tiered” system (Health Policy Partnership on weight loss treatment inequalities).
That has created two very different patient experiences.
- Some patients get structured care: They have proper screening, follow-up, dose adjustment, and clinical oversight.
- Others get a pen and very little else: No one checks whether the medicine suits them, whether side effects are becoming unsafe, or whether the weight they’re losing is healthy weight to lose.
The key difference is supervision
The excitement around these medicines is justified. The casual way they’re sometimes marketed is not.
Practical rule: A weight loss injection is only as safe as the medical programme around it.
A responsible approach starts with diagnosis and selection. It continues with monitoring, nutrition support, and a plan for what happens if symptoms appear, progress stalls, or weight begins to return.
That matters because obesity care isn’t just about appetite. It touches cardiovascular risk, liver health, mobility, sleep, energy, and mental wellbeing. Patients need treatment that reflects that full picture.
For people considering a private weight loss clinic, the best option is not the fastest checkout process. It’s the setting where a clinician looks at the whole patient and treats weight as a medical issue, not an online retail transaction. Blood tests, regular check ins and consideration of previous health issues are all key to ensuring long term weight loss goals are achieved in a way that won’t compromise your overall health.
How Do Weight Loss Injections Work
Individuals typically don’t need a lecture in hormone physiology. They need a clear explanation of why these medicines change eating behaviour in a way willpower alone often doesn’t.
A useful way to think about them is this. They help turn down the volume on hunger and turn up the body’s sense of fullness.
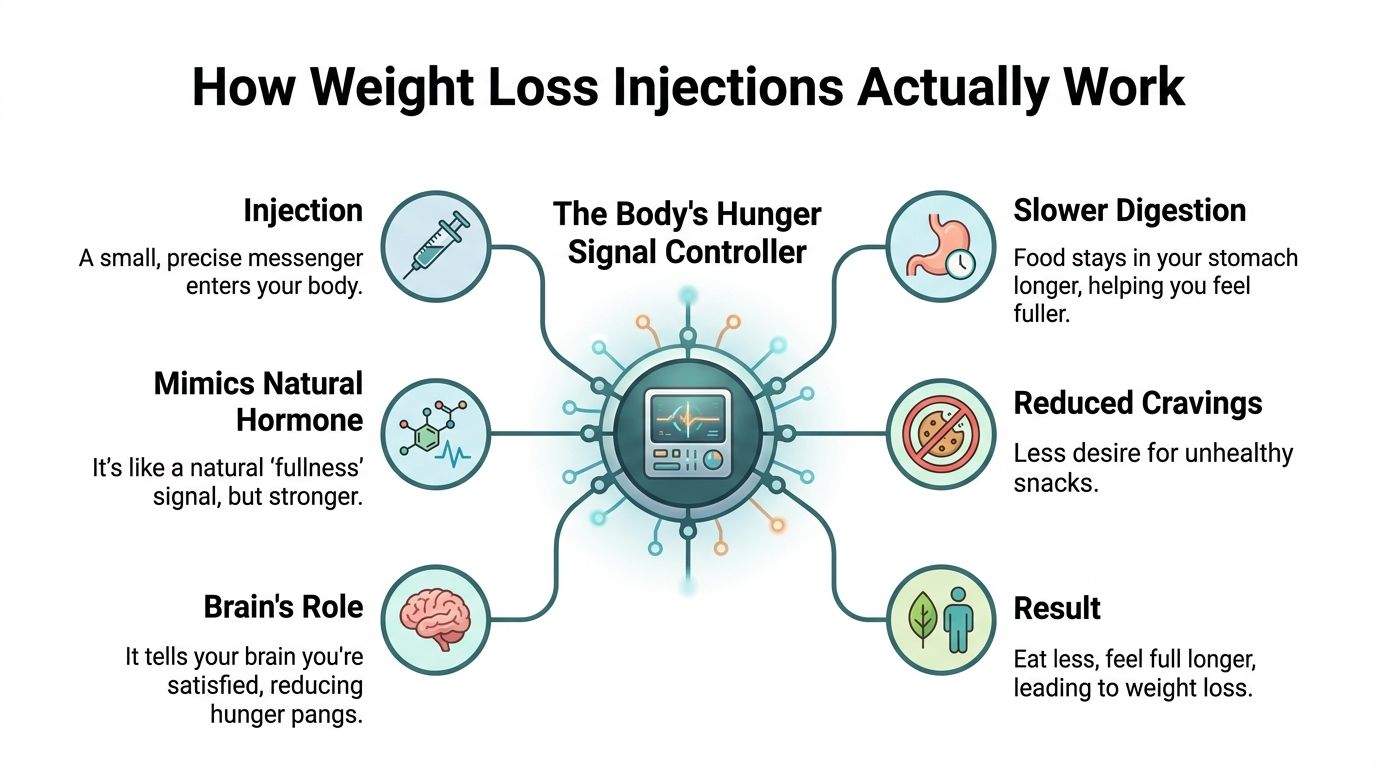
The GLP-1 pathway in plain English
Medicines such as semaglutide UK patients may hear about work by mimicking a natural hormone pathway involved in appetite and glucose regulation.
In practice, patients usually notice effects such as:
- Less constant hunger: Food isn’t on the mind all day.
- Earlier fullness: Portions that once felt small can feel sufficient.
- Reduced snacking pull: Cravings often become quieter and easier to resist.
- Better control around meals: Eating feels more deliberate and less reactive.
There are also digestive effects. Food moves more slowly through the stomach, which can help prolong satiety. That’s one reason some people feel fuller for longer, but it’s also one reason nausea can occur if dose increases happen too quickly or eating habits don’t adjust.
Why tirzepatide is different
Tirzepatide UK treatment builds on the same general principle but uses a dual pathway. It targets both GLP-1 and GIP receptors, rather than a single pathway alone.
That dual action matters clinically because it appears to improve insulin sensitivity and appetite control more strongly than single-pathway treatment. In the head-to-head data reported in the SURMOUNT-5 trial, tirzepatide achieved mean weight loss of 20.2% compared with 13.7% for semaglutide over 72 weeks, with stronger response at higher weight-loss thresholds as well (SURMOUNT-5 comparative data in PMC).
What patients often notice first
The first meaningful change is not always the scales. It is often the reduction in mental effort around food.
Many patients describe the earliest benefit as quieter food thoughts rather than dramatic weight change in the first few weeks.
That shift can be powerful, but it doesn’t remove the need for medical judgement. The same mechanism that reduces appetite can also make it easier to under-eat protein, skip meals in an unhelpful way, or push through side effects instead of addressing them.
These medicines work best when the biology and the behaviour are managed together. The injection helps create the opportunity. The treatment plan determines whether that opportunity turns into safe, durable progress.
Comparing the Leading Weight Loss Injections UK Patients Can Access
A new patient will often come in asking a very direct question. “Which injection works better?” My answer is usually that the better medicine is the one that produces meaningful weight loss, is tolerated well enough to continue, and is prescribed within a properly supervised treatment plan.
In private UK practice, the two medicines patients ask about most are semaglutide (Wegovy) and tirzepatide (Mounjaro). Both are once-weekly injections. Both can be effective. The choice between them depends on more than the headline weight-loss figure.
Semaglutide vs tirzepatide at a glance
| Feature | Semaglutide (Wegovy) | Tirzepatide (Mounjaro) |
|---|---|---|
| Drug type | GLP-1 receptor agonist | Dual GLP-1 and GIP receptor agonist |
| Dosing | Weekly injection | Weekly injection |
| Average body weight reduction | 13.7% | 20.2% |
| Typical clinical appeal | Often a sensible starting option for patients who want a steady, structured approach | May suit patients where greater weight-loss efficacy is appropriate |
| Main prescribing considerations | Tolerability, treatment goals, coexisting conditions, pace of dose escalation | Tolerability, treatment goals, coexisting conditions, pace of dose escalation |
The commonly quoted comparison figures above, along with reports of improved quality of life after several months of treatment, are summarised in these UK weight loss injection statistics.
What the comparison means in practice
Tirzepatide has shown greater average weight reduction in comparative data. That matters, particularly for patients with obesity-related health risks where a larger reduction may bring greater clinical benefit.
But prescribing is never as straightforward as picking the strongest option on paper.
Some patients do well with a slower, steadier approach and prefer the track record of semaglutide. Some are more sensitive to gastrointestinal side effects and need cautious dose escalation. Others need close support with protein intake, hydration, and meal structure because once appetite drops, poor habits can hide behind early weight loss. Tools such as a GLP-1 protein calculator can help patients meet basic nutritional targets, but they do not replace medical review.
Trade-offs Patients Should Understand
Semaglutide may be the better fit when:
- a patient wants a simpler starting point with gradual escalation
- previous response to a GLP-1 medicine has been acceptable
- tolerability and consistency matter more than pursuing the highest possible average weight-loss result
Tirzepatide may be the better fit when:
- a patient has a higher clinical need for substantial weight reduction
- appetite control has been poor despite other structured efforts
- the patient understands the likely benefits, side effects, monitoring needs, and cost implications
Here, the difference between obtaining an injection and entering a weight loss programme led by a GP becomes very clear.
A prescription on its own does not assess whether the target weight is realistic, whether nausea is causing under-eating, whether constipation is becoming significant, or whether rapid loss is coming at the expense of muscle mass and long-term adherence. A medically supervised programme does. It also gives patients somewhere to turn when treatment needs adjusting, pausing, or stopping.
The right injection is not the one associated with the biggest number. It is the one that fits the patient safely, can be sustained, and sits within proper clinical follow-up.
Both medicines have a place in private obesity care. The better choice is the one selected with judgement, monitoring, and a clear plan for what happens after the first few months.
More Than Weight Loss The Long-Term Health Benefits
The most important reason to take obesity treatment seriously is that excess weight affects far more than appearance. It changes cardiovascular risk, metabolic function, liver health, mobility, inflammation, and future disease burden.
That is why medically supervised treatment should never be framed as vanity care.

The benefits go well beyond the scales
A large UK analysis published through the British Heart Foundation compared approximately 215,000 people with diabetes prescribed weekly GLP-1 agonist injections with over 1.2 million people on standard non-GLP-1 blood sugar medicines over an average follow-up of 3.68 years. It found a 22% lower risk of cardiac arrest, 11% lower risk of heart failure, 9% lower risk of heart attack, and 7% lower risk of ischaemic stroke among GLP-1 users. The same analysis also reported a 24% reduced likelihood of liver failure, 22% lower chance of respiratory failure, and 12% decreased risk of developing Alzheimer’s disease (British Heart Foundation review of weight loss injection evidence).
Those are serious outcomes. They shift the discussion away from dress size and toward risk reduction.
Why supervision improves the value of treatment
The weight loss itself is not the whole story. What matters is using that weight loss to improve health in a durable way.
A clinician-led programme can keep the focus on:
- Cardiometabolic improvement: Blood sugar patterns, blood pressure, and overall cardiovascular risk.
- Functional gain: Easier walking, better sleep, less joint strain, and better day-to-day energy.
- Protection against poor-quality loss: Preserving muscle and nutritional status while body fat falls.
Patients often benefit from practical tools that support good nutrition while appetite is reduced. If you’re trying to keep protein intake adequate during treatment, a GLP-1 protein calculator can be a useful starting point for meal planning discussions with your clinician.
Benefits still come with trade-offs
Benefits still come with trade-offs. Honest medicine is important. The same BHF summary that reported broad health benefits also noted important risks, including being nearly 2.5 times more likely to develop drug-induced acute pancreatitis, alongside a 30% higher risk of nausea or vomiting, 11% increased arthritis risk, and 6% higher chance of low blood pressure.
That doesn’t make the treatment unsafe by default. It means the treatment needs context, screening, and monitoring.
These medicines can improve long-term health substantially, but they are safest when a doctor is watching the whole patient, not just the weekly weight reading.
Why a Programme Led by a GP Matters
A patient comes to see me after ordering injections online. The appetite suppression is strong, the scales are down, and on the surface it looks successful. Then the fuller picture emerges. She feels weak, is skipping meals, drinking very little, and has had no one check whether the treatment suits her medical history or whether the weight coming off is body fat, muscle, or both.
That is the difference between getting hold of an injection and being treated properly.
These medicines have real physiological effects. They can reduce appetite, improve control around eating, and help with weight reduction. They also change how much you eat, how well you tolerate food, how hydrated you stay, and whether you maintain muscle while losing weight. Without clinical oversight, people can mistake rapid weight change for good progress.
The hidden problem of poor-quality weight loss
Lower appetite creates practical problems that many patients do not anticipate. If food intake drops sharply and meals become irregular, protein intake often falls first. Strength activity is also commonly reduced because patients feel tired, light-headed, or under-fuelled.
The result can be weight loss with too much lean mass loss alongside it.
Patients usually notice this as reduced strength, poorer stamina, and a sense that they are smaller but not healthier. If you use home measurements, it also helps to understand results from a body fat scale properly, because a lower number on the scales does not automatically mean better body composition.
What a GP adds
A doctor’s role is broader than writing a prescription. The job is to decide whether treatment is appropriate, make sure there is a sound reason to use it, check for risks and contraindications, and monitor whether the balance of benefit and harm remains acceptable.
That means asking different questions from a simple online checkout.
Screening before treatment starts
Some patients are suitable candidates. Others need further assessment, a different approach, or treatment for another problem first.
A proper review looks at medical history, current medicines, eating patterns, gastrointestinal symptoms, previous attempts at weight reduction, mental health, and the possibility that weight change is linked to another condition.
Managing side effects before they become setbacks
Nausea, vomiting, constipation, dehydration, dizziness, and poor oral intake are common reasons patients struggle. These are not minor details. If symptoms persist, the dose may need to stay where it is, be reduced, or the treatment may need to stop.
Good care involves active follow-up, practical dietary advice, and clinical judgement about whether the medicine is still the right fit. Blood tests may be recommended to check key blood components, such as iron levels.
Protecting muscle and nutrition
This is often where unsupervised treatment falls short. Patients need clear advice on protein, meal structure, hydration, bowel habits, and resistance exercise. Appetite suppression is not a licence to eat as little as possible.
I often tell patients a simple truth. Deliberate eating matters more once hunger becomes less reliable.
Patterns that cause problems
The same mistakes come up repeatedly in clinic:
- Starting medication after only minimal screening
- Pushing the dose up because weekly loss has slowed
- Ignoring ongoing side effects because the scales are improving
- Paying attention to calories but not food quality
- Stopping suddenly without any plan for maintenance or regain prevention
A programme led by a GP is not red tape. It is the structure that keeps treatment safer, helps preserve health while weight falls, and gives you a better chance of maintaining the result rather than chasing short-term loss at any cost.
Your Journey with a Private Weight Loss Clinic
Patients often feel less anxious once they understand what proper treatment looks like. The process should be calm, structured, and personalised. It should not feel like buying a product from a checkout page.

The first appointment
The opening consultation is about understanding the full picture. Why has weight become difficult to manage now? What has already been tried? What other health concerns sit around it?
This conversation should cover:
- Medical background: Existing conditions, symptoms, medicines, and relevant family history.
- Weight history: Patterns of gain, previous losses, and what happened afterwards.
- Treatment goals: Some patients want improved mobility. Others want better metabolic health or fewer food cravings. Often it is a combination.
The assessment stage
Not every patient needs the same checks, but proper assessment matters. It creates a baseline and helps the clinician prescribe with more confidence.
A thoughtful assessment may include general health review, relevant measurements, and investigations where indicated. It also gives the patient a realistic idea of what treatment can and cannot do.
Choosing the treatment plan
Once suitability is clear, the plan becomes specific, and prescribing decisions for semaglutide UK or tirzepatide UK should be individualised.
A strong plan usually sets out:
- Which medication is being used
- How dose escalation will happen
- What side effects to expect
- What to do if eating becomes difficult
- What markers define success beyond weight alone
Some patients also benefit from learning how to interpret body composition readings properly. If you’re using home scales and want to better understand results from a body fat scale, that can help frame sensible discussions during follow-up rather than relying on one number in isolation.
Follow-up is where outcomes are protected
The middle phase of treatment is where most of the important work happens. Dose changes, appetite changes, food tolerance, bowel symptoms, hydration, and energy all need periodic review.
A good follow-up process gives room to ask practical questions such as:
- Am I eating enough protein?
- Is this level of nausea acceptable or not?
- Should my dose stay where it is?
- Why has my weight loss slowed?
- How do I maintain progress without becoming undernourished?
Planning for maintenance
Long-term success doesn’t come from reaching a certain dose. It comes from deciding how weight, appetite, health markers, and habits will be managed over time.
That may mean staying on treatment, adjusting strategy, or moving into a maintenance phase with closer attention to nutrition and activity. The exact route varies, but the principle stays the same. Treatment should remain purposeful, not automatic.
Your Questions Answered About Safe Weight Loss Injections
Can I take these injections if I’m not diabetic
Yes, these medicines are not only used in diabetes care. In weight management, the key issue is whether the treatment is clinically appropriate for your health profile and goals. That decision should be made by a prescribing clinician after proper assessment, not by self-selection online.
What happens when I stop the injections
Weight regain can happen after stopping. That is one reason obesity treatment should be approached as long-term medical care rather than a short burst of intervention. If treatment is ever reduced or stopped, patients need a maintenance strategy instead of hoping appetite and weight regulation will remain unchanged.
How long will I need to stay on them
There isn’t one answer for everyone. Some patients need longer treatment to maintain benefit. Others may eventually change plan depending on response, side effects, or wider health priorities.
The important point is that duration should be reviewed clinically. It should not be based on how long a pen lasts, how quickly someone wants results, or whether a friend stopped after a certain number of months.
Are these injections safe
They can be safe and effective when prescribed appropriately and monitored properly. They are not risk-free.
The safest approach includes assessment before starting, dose titration with oversight, regular review, and active support around nutrition, symptoms, and maintenance. That is what turns a prescription into proper care.
What is the most sensible next step
If you’re considering weight loss injections UK treatment, look for a clinician-led service that treats obesity as a medical condition and not as a quick online purchase. The medicine matters, but the supervision matters just as much.
Weight loss by injection can be a powerful option. It can reduce hunger, support meaningful weight loss, and improve long-term health. But it works best inside a structured plan that protects muscle, nutrition, and safety while aiming for lasting change.
If you’re ready for a careful, personalised discussion about whether treatment is right for you, book a consultation with Haven Medical. You can click to book an appointment with one of our GPs or call 01202 110303 today.